ENT
2 questionsHot potato voice is characteristic of ?
What is not true about the use of intranasal steroids in nasal polyposis?
Internal Medicine
3 questionsA 40-year-old male patient presents to the Emergency department with central chest pain for 2 hours. The ECG shows ST segment depression and cardiac troponins are elevated. The patient has a positive history of previous PCI 3 months back. He is administered Aspirin, Clopidogrel, Nitrates, and LMWH in the Emergency Department and shifted to the coronary care unit. What is the best recommended course of further action?
What is the most common cause of lobar consolidation?
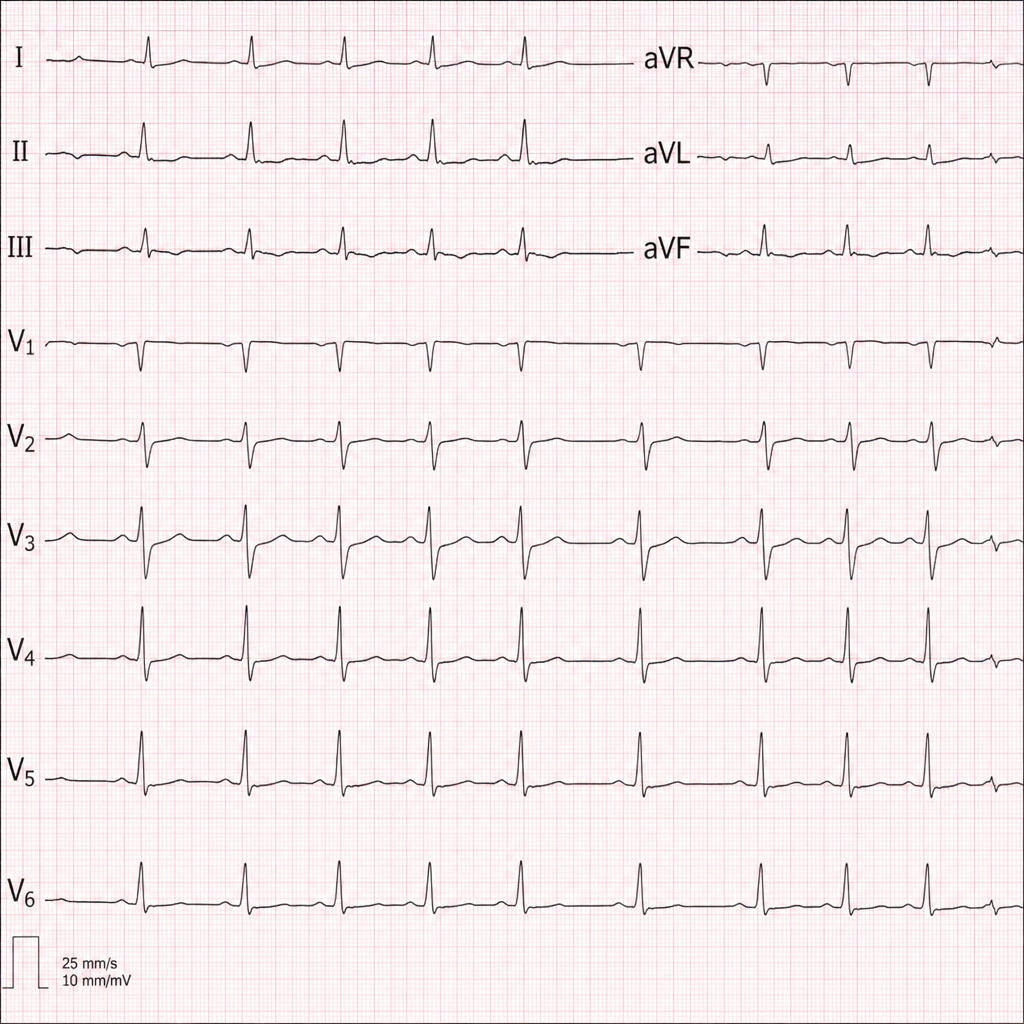
Diagnose the underlying medical disorder based on the ECG changes.
Ophthalmology
2 questionsCicatrising trachoma is associated with which stage of the disease?
Arcuate field defect akin to glaucoma is seen in?
Orthopaedics
2 questionsMost commonly recommended cast position for proximal forearm fractures is ?
Garden spade deformity is seen in ?
Pathology
1 questionsWhat are the common causes of vertebra plana?