Biochemistry
1 questionsWhich gene is responsible for the production of COX type 3?
Forensic Medicine
1 questionsBase of sphenoid fuses with occiput at the age of -
Internal Medicine
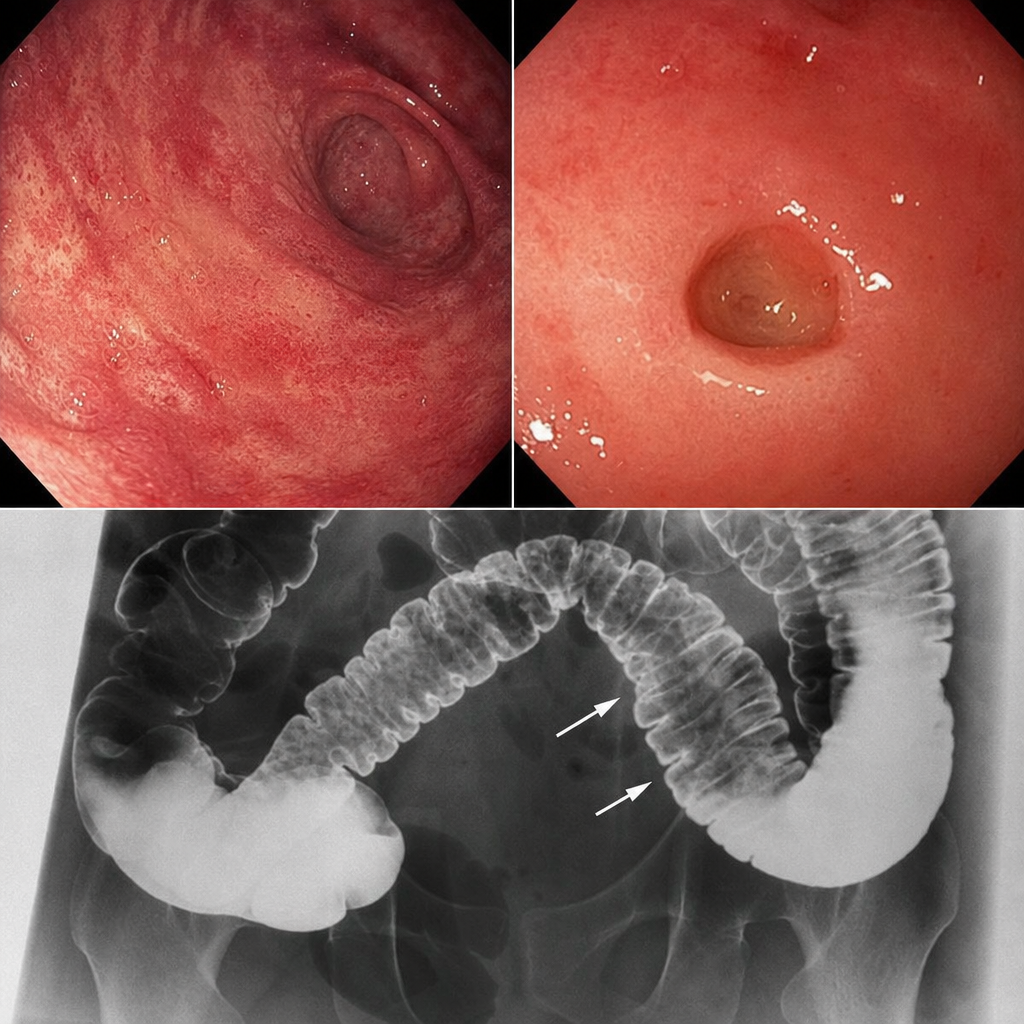
1 questionsA patient presents with skin involvement and collar stud ulceration in the intestine observed on radiography. What is the most likely diagnosis?
Pathology
2 questionsWhich genetic condition is considered the most lethal due to monosomy?
Obliterative endarteritis in vasa vasorum is seen in -
Pharmacology
3 questionsWhich of the following agents requires the MOST caution when combined with spironolactone due to increased risk of hyperkalemia:
What is the drug of choice for drug-induced peptic ulcer?
Which of the following is an action of muscarinic cholinergic receptors?
Physiology
2 questionsRebound increase in gastric acid secretion after stopping proton pump inhibitor therapy is due to?
'Flare' in Triple response is mediated by :