All (1417)Anatomy (167)Anesthesiology (9)Biochemistry (108)Community Medicine (87)Dental (8)Dermatology (19)ENT (30)Forensic Medicine (62)General Medicine (3)Internal Medicine (136)Microbiology (101)Obstetrics and Gynecology (65)Ophthalmology (60)Orthopaedics (33)Pathology (107)Pediatrics (37)Pharmacology (123)Physiology (116)Psychiatry (2)Psychiatry (38)Radiology (25)Surgery (81)
Pharmacology
1 questionsQ1311
Which of the following is the only clinically available depolarizing muscle relaxant?
Psychiatry
4 questionsQ1311
Which drug is not considered a mood stabilizer?
Q1312
What is the most common cause of delirium?
Q1313
Increased dopamine levels are associated with which of the following conditions?
Q1314
What does the term 'jamais vu' refer to?
Radiology
4 questionsQ1311
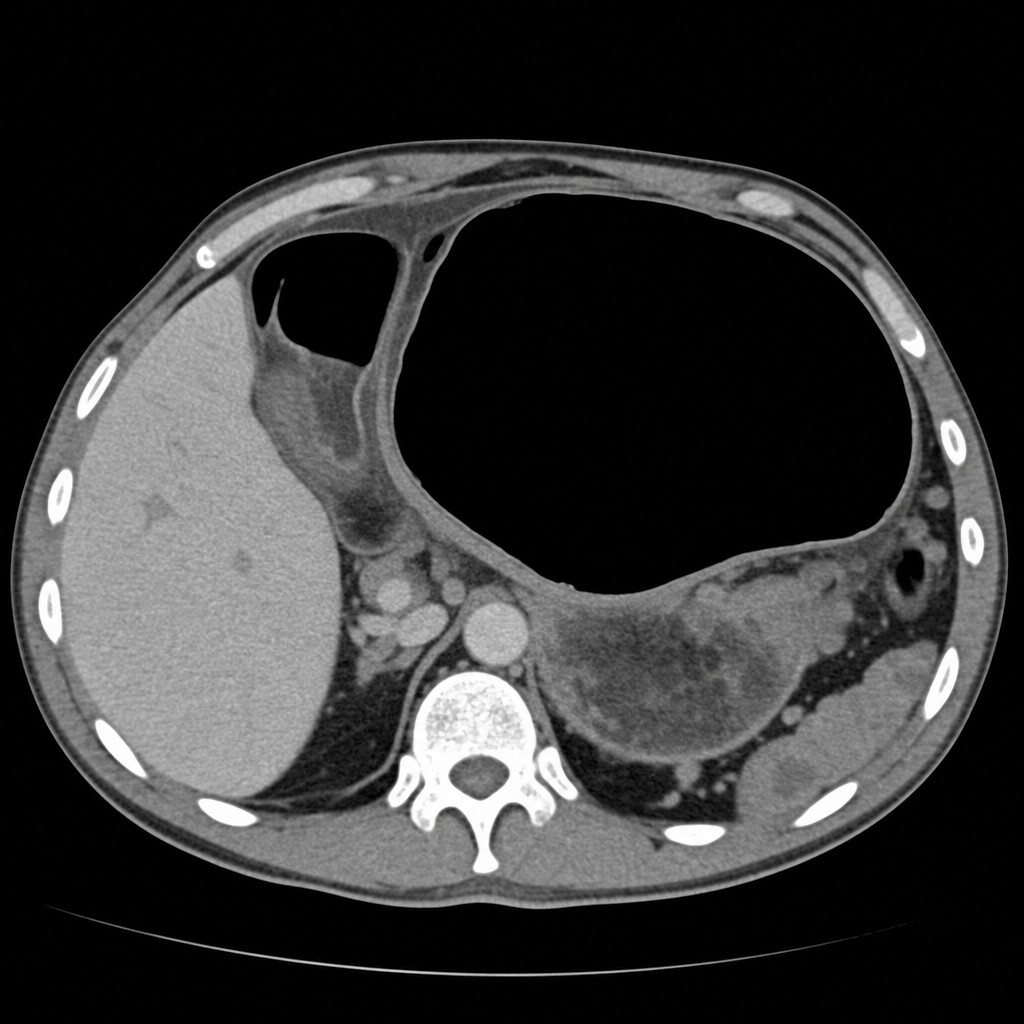
On CT scan, gastric volvulus typically shows which of the following findings?
Q1312
Epidural hematoma on CT scan shows which of the following?
Q1313
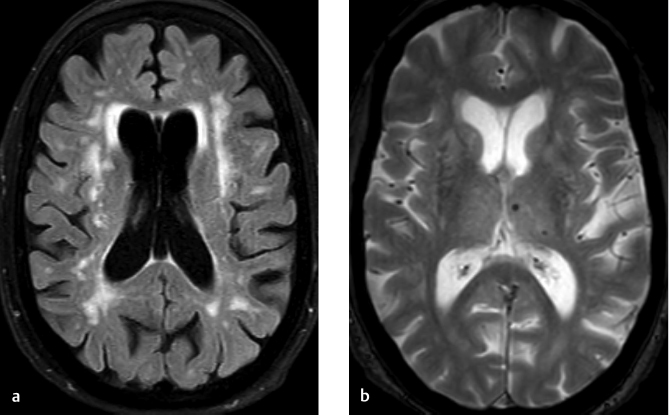
Tigroid pattern on MRI is seen in -
Q1314
Which of the following X-ray findings is associated with Chilaiditi syndrome?
Surgery
1 questionsQ1311
A patient presents with abdominal pain. On physical examination there was abdominal guarding and tenderness. A plain erect chest X-ray reveals air under diaphragm. Probable diagnosis is
