What is the immediate emergency treatment for carbon monoxide (CO) poisoning?
Which of the following is not a feature of Poststreptococcal Glomerulonephritis (PSGN)?
Which type of thyroid cancer is associated with primary hyperparathyroidism and phaeochromocytoma?
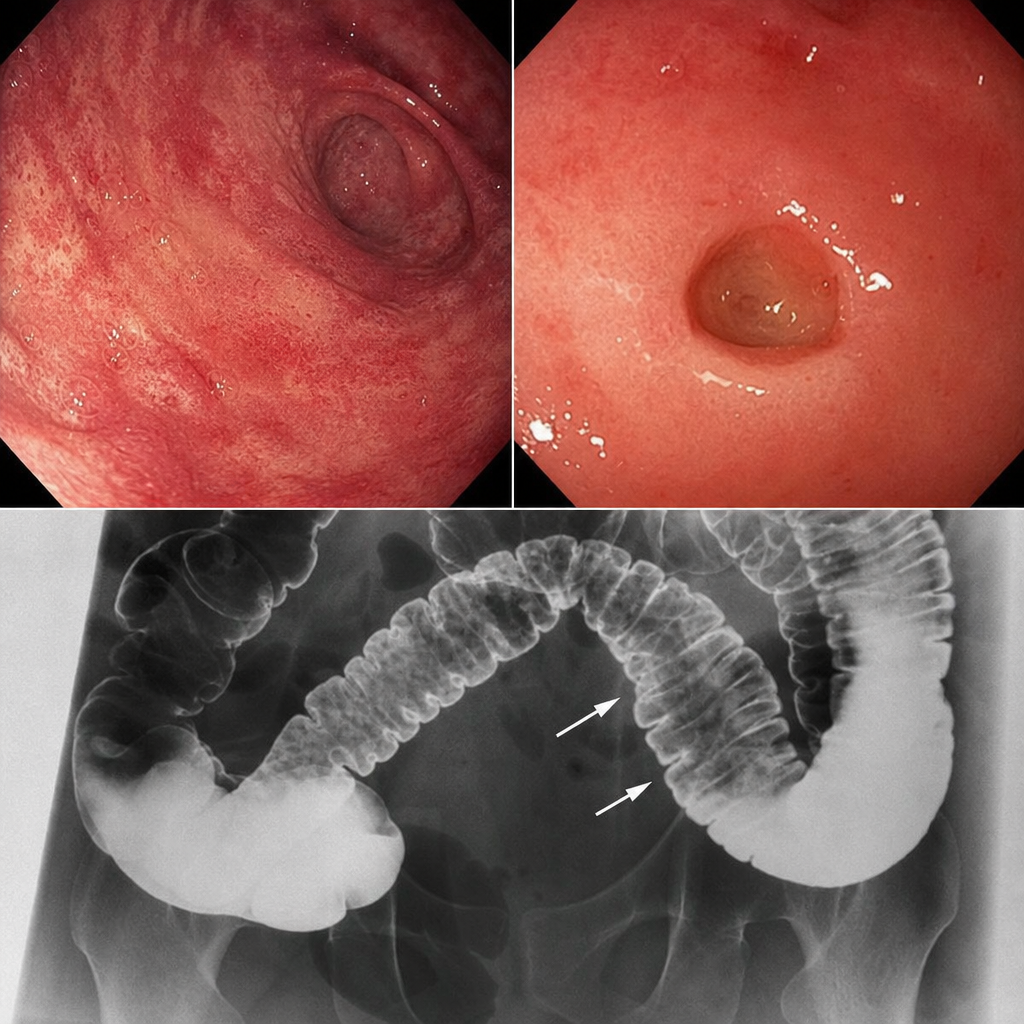
A patient presents with skin involvement and collar stud ulceration in the intestine observed on radiography. What is the most likely diagnosis?
In which condition is the Doll's Eye Reflex tested?
Which subtype of Acute Myeloid Leukemia (AML) is associated with the best prognosis?
In which condition is Serum Amyloid Associated (SAA) protein most commonly found?
Shrinking Lung Syndrome is seen in:
What is the primary effect of beta blockers in the management of thyroid storm?
Extremities are warm in which type of shock