All (1550)Anatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Anesthesiology
2 questionsQ1301
Who coined the term "balanced anaesthesia"?
Q1302
Which of the following anesthetics is known to increase intraocular pressure?
Dermatology
3 questionsQ1301
The Grattage test is used to diagnose which of the following conditions?
Q1302
Pathergy test is used for which condition?
Q1303
A man with pain during defecation, no gastrointestinal symptoms, and ulcers extending into the anal canal. Diagnosis?
Internal Medicine
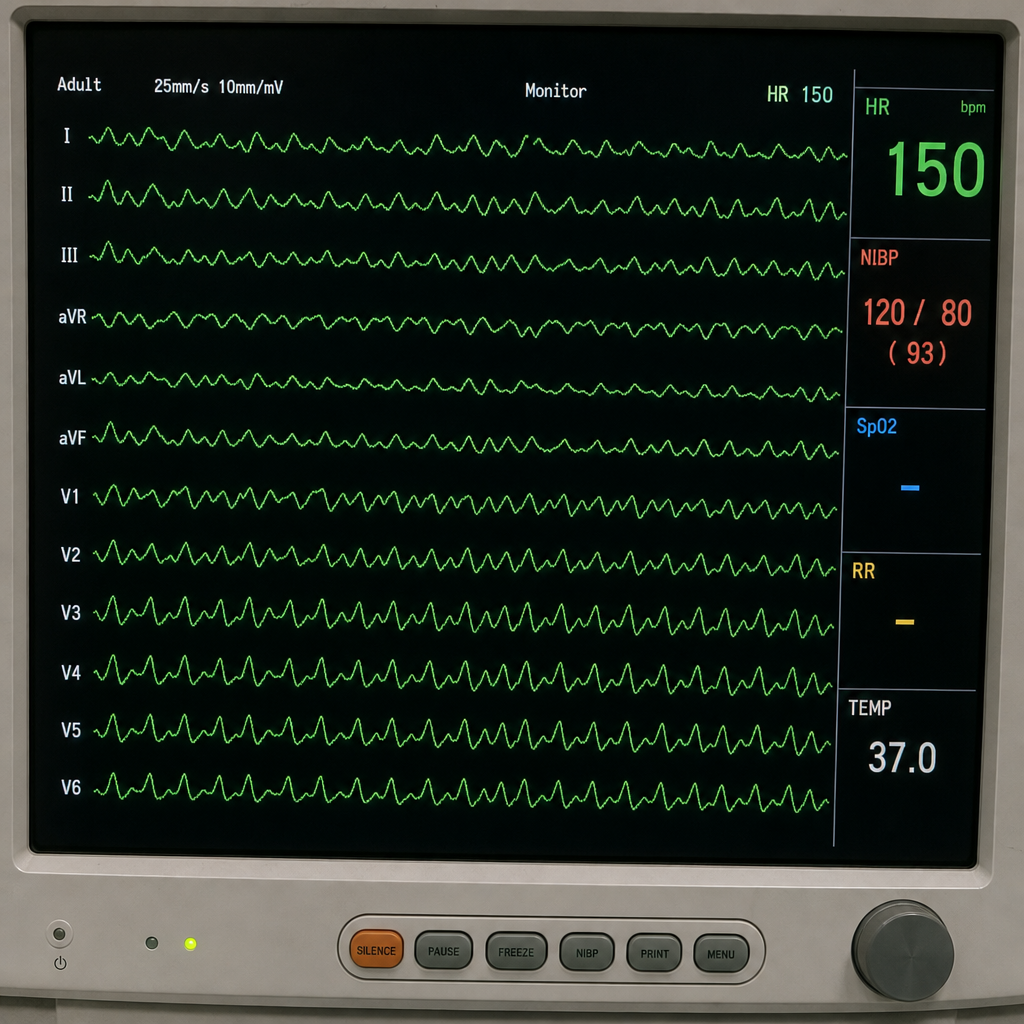
1 questionsQ1301
Refer to the provided ECG image. It demonstrates which of the following?
Pathology
1 questionsQ1301
Which of the following statements about chronic osteomyelitis is false?
Pharmacology
1 questionsQ1301
Which of the following medications is not typically used for the treatment of erectile dysfunction?
Radiology
1 questionsQ1301
Which of the following is NOT a typical differential diagnosis for a solitary pulmonary nodule?
Surgery
1 questionsQ1301
Pulled up cecum is seen in which condition?