Anatomy
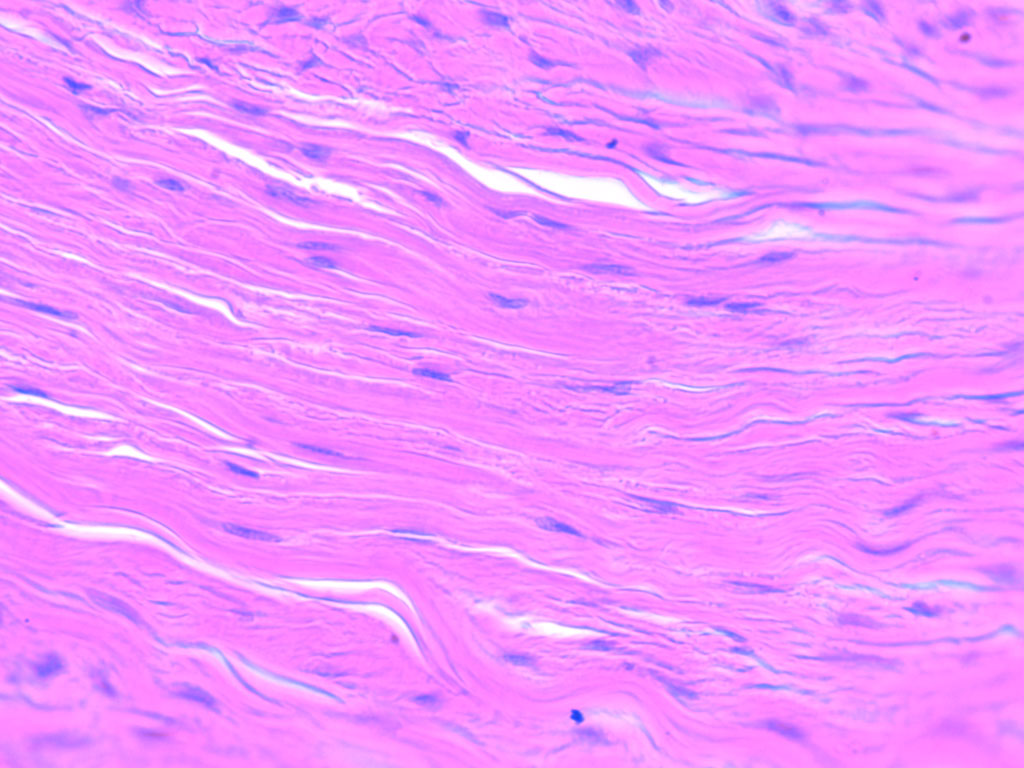
1 questionsIdentify the type of connective tissue present in the image.
Anesthesiology
1 questionsAyre's T-piece is which type of circuit
Dermatology
1 questionsWhat is the maximum cumulative dose of isotretinoin for acne treatment?
Internal Medicine
1 questionsWhat is the initial drug of choice for a suspected case of acute adrenal insufficiency?
Obstetrics and Gynecology
1 questionsAll are causes of anovulatory amenorrhea except which of the following?
Pediatrics
2 questionsA child presents with recurrent pulmonary infections and hemoptysis due to associated bronchiectasis. Imaging shows unilateral loss of lung volume with hyperlucency on chest radiograph and reduced vascularity on CT scan of the chest. The abdominal organs are normally placed. What is the most likely cause?
What is the most common complication of a large Patent Ductus Arteriosus (PDA)?
Radiology
1 questions"Sunray appearance" on X-rays is suggestive of:
Surgery
2 questionsDiversion of urine is best done at
What is the most reliable diagnostic tool to differentiate between psychological and organic erectile dysfunction?