All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Anatomy
2 questionsQ171
Ovarian fossa is formed by all except?
Q172
Which of the following is NOT an anterior relation of the right kidney?
Biochemistry
5 questionsQ171
Which of the following is a termination codon?
Q172
What is the primary function of reverse transcription?
Q173
Km value is defined as:
Q174
Which enzyme catalyzes the rate limiting step in the TCA cycle?
Q175
Which tissue cannot convert glucose 6-phosphate to free glucose due to lack of glucose-6-phosphatase?
Internal Medicine
1 questionsQ171
Which type of fatty acids should be included in the diet to manage chyluria?
Pathology
1 questionsQ171
Which of the following does not belong to the family of selectins?
Physiology
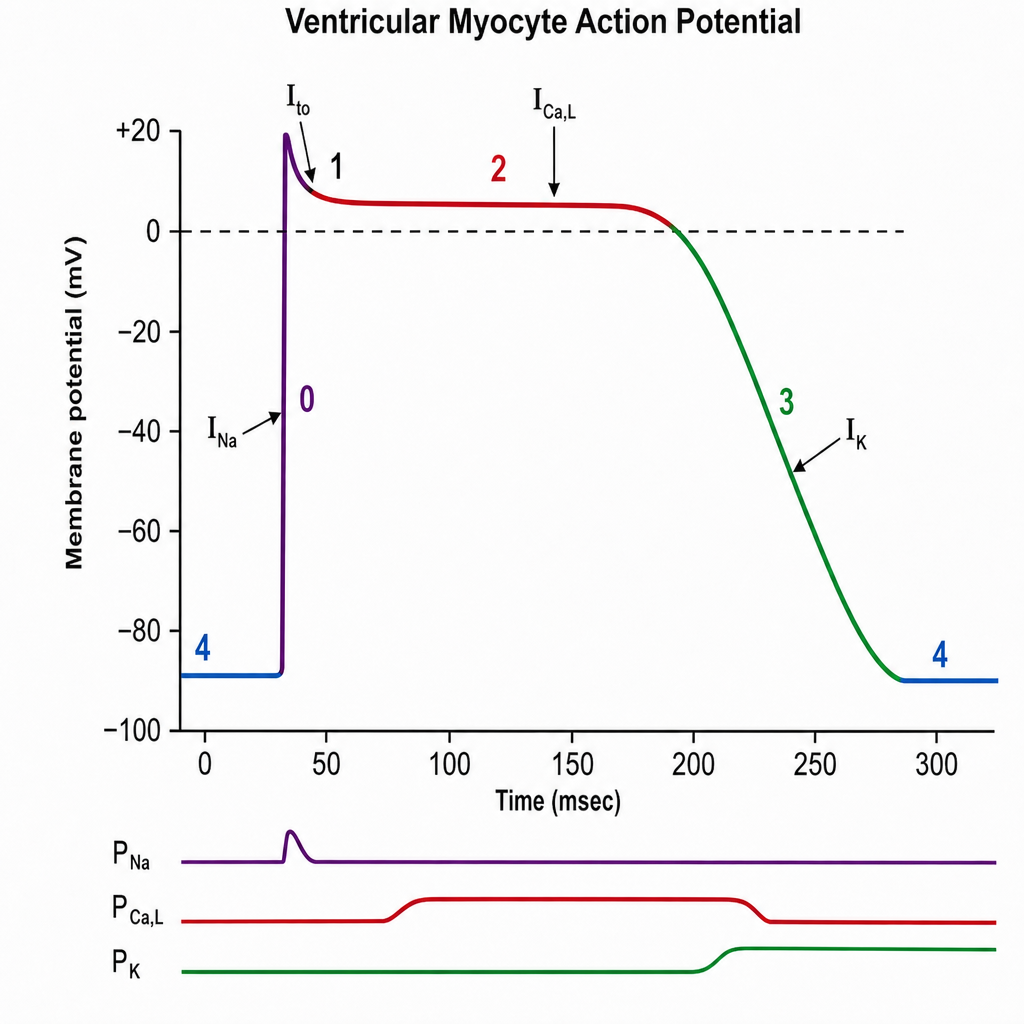
1 questionsQ171
The plateau phase of this graph is due to: