Anatomy
1 questionsWhich statement accurately describes a characteristic of synovial joints?
Biochemistry
5 questionsWhich of the following statements about protein denaturation is correct?
Acute intermittent porphyria is due to deficiency of?
The primary site of lipogenesis is:
Which amino acid among the following has significant UV absorption at 280 nm used in protein quantification?
What does Chargaff's rule state regarding the base pairing in DNA?
Physiology
4 questionsWhich of the following is most important in sodium and water retention ?
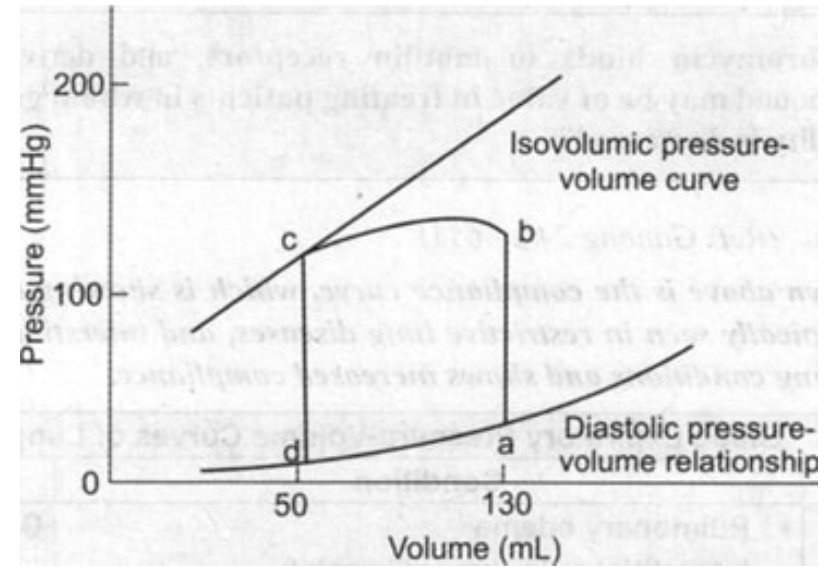
From the given pressure-volume curve, identify the end-diastolic volume (EDV) and end-systolic volume (ESV), then calculate the ejection fraction using the formula EF = (EDV - ESV)/EDV × 100%.
What is the process by which water moves from the extracellular space to the intracellular space?
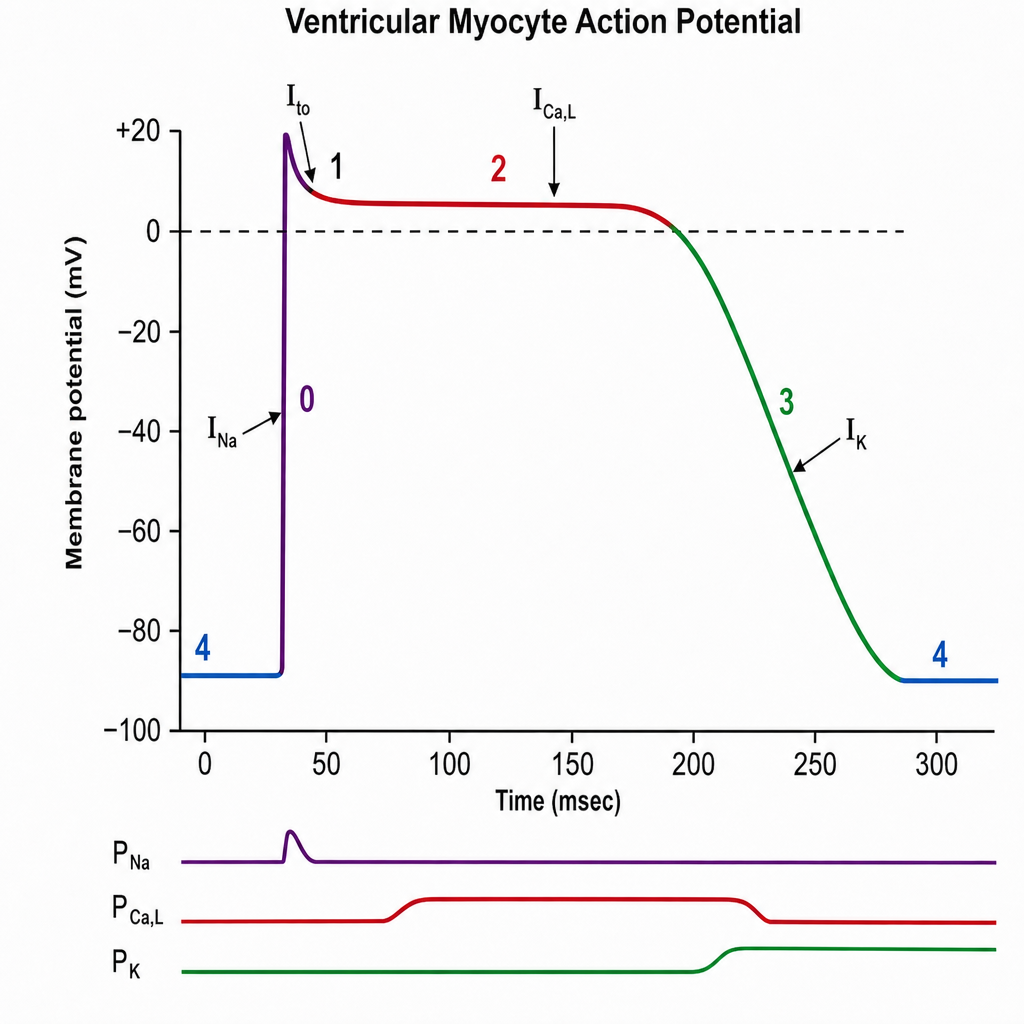
The plateau phase of this graph is due to: