All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Biochemistry
5 questionsQ151
The primary defect which leads to sickle cell anemia is:
Q152
Which of the following is not a precursor in the synthesis of pyrimidines?
Q153
In the electron transport chain (ETC), which enzyme does cyanide inhibit?
Q154
What is the rate-controlling enzyme of fatty acid synthesis?
Q155
Methionine can enter the TCA cycle at which level?
Pathology
1 questionsQ151
Nutmeg liver is associated with which condition?
Physiology
3 questionsQ151
What is the normal range for the CSF/plasma glucose ratio?
Q152
Which of the following is the MOST accurate statement about CSF?
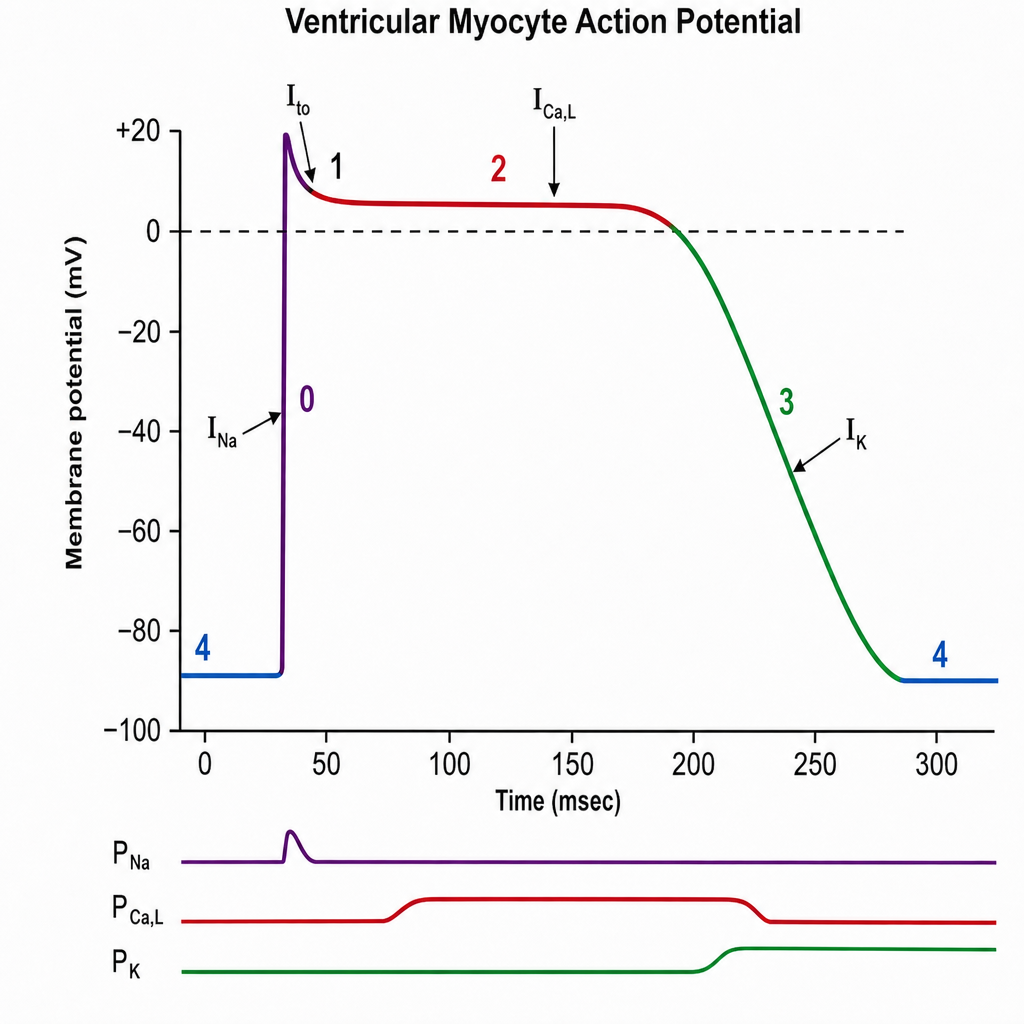
Q153
The plateau phase of this graph is due to:
Surgery
1 questionsQ151
IVC filter is used in the following situations except -