All (1216)Anatomy (104)Anesthesiology (21)Biochemistry (179)Community Medicine (104)Dental (9)Dermatology (21)ENT (2)Forensic Medicine (41)General Medicine (2)Internal Medicine (79)Microbiology (83)Obstetrics and Gynecology (63)Ophthalmology (68)Orthopaedics (36)Pathology (82)Pediatrics (43)Pharmacology (85)Physiology (91)Psychiatry (2)Psychiatry (20)Radiology (28)Surgery (53)
Anesthesiology
1 questionsQ1011
Fast induction and recovery is seen in?
Internal Medicine
1 questionsQ1011
Best provocative test for diagnosis of Gastrinoma is:
Obstetrics and Gynecology
3 questionsQ1011
After delivery upto which week is known as puerperium?
Q1012
Which of the following pelvic measurements is most commonly used in clinical practice?
Q1013
What is thelarche?
Orthopaedics
3 questionsQ1011
Sequestrum is best defined as
Q1012
What is the most common complication associated with carpal tunnel release surgery?
Q1013
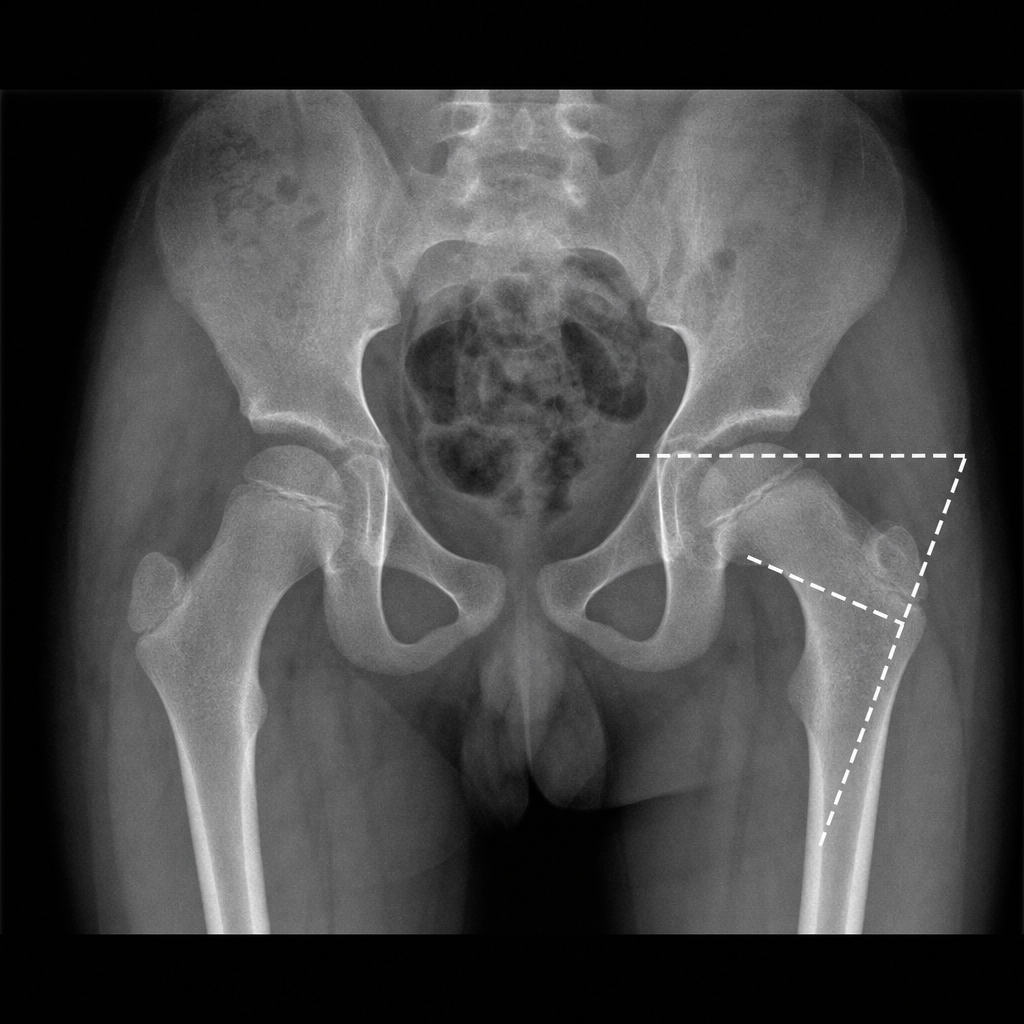
Fairbank triangle is seen in
Pathology
1 questionsQ1011
Most common CNS tumor associated with NF1
Psychiatry
1 questionsQ1011
What does the term 'etheromania' refer to?