Biochemistry
1 questionsAn adult tall male presents with a long arm span, pectus excavatum, and cardiac abnormalities. What is the most likely defective protein?
ENT
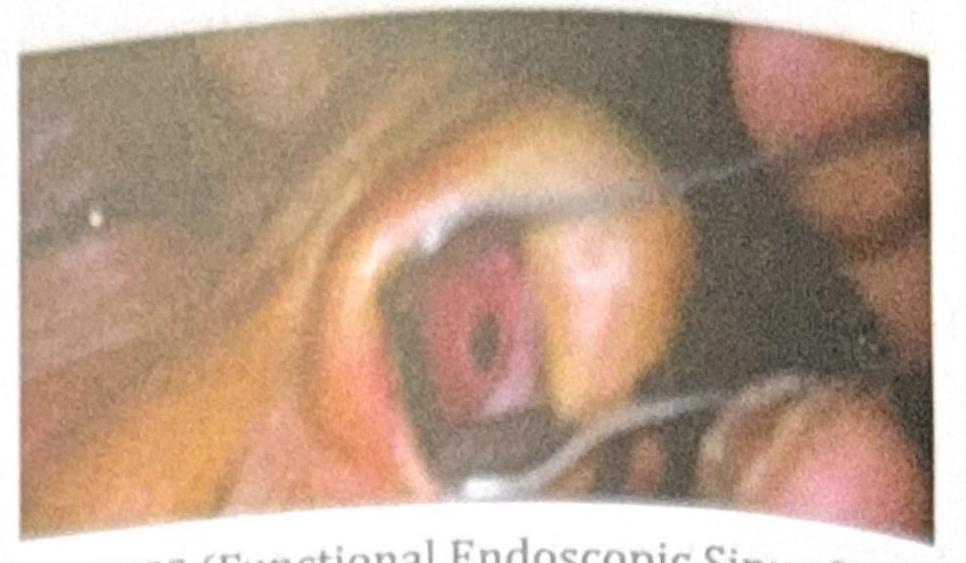
4 questionsA nasal surgery was carried out with the incision shown in the image. What was the procedure likely carried out?

In a patient with right vestibular neuronitis, what will be the finding on the head impulse test?
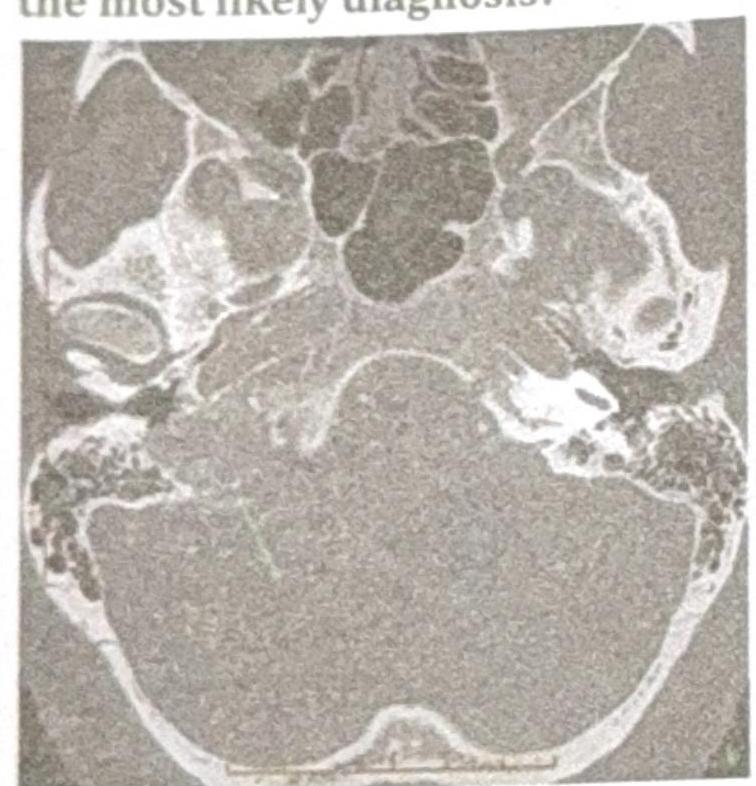
A patient presents with conductive hearing loss, pulsatile tinnitus, and a positive Phelps sign. Based on the CT scan image provided, what is the most likely diagnosis?
A patient with chronic nasal obstruction underwent a procedure 3 months ago and now presents with recurrent epistaxis, crusting, and the clinical image showing a septal perforation. What procedure was most likely carried out?
Internal Medicine
1 questionsA 32-year-old female presents with a 2-month history of progressive, painless swelling in the left side of her neck. She also reports low-grade fever, night sweats, and unintentional weight loss. Physical examination reveals a firm, non-tender, immobile mass in the left cervical region, and multiple smaller lymph nodes in the supraclavicular area. Chest X-ray shows mediastinal widening, and a lymph node biopsy confirms the presence of Reed-Sternberg cells. What is the most appropriate management for this patient?
Pathology
2 questionsWhich of the following is an intracellular marker or deposition found in Alzheimer's disease?
A patient presents with headaches, palpitations, hypertension, and urine VMA positivity. The biopsy findings are shown in the image. Which of the following statements is correct?
Pediatrics
1 questionsA child presents with recurrent infections. Mediastinal imaging reveals an absent thymus gland, and further investigations show low ADA (adenosine deaminase) levels. What is the most likely diagnosis?
Surgery
1 questionsWhich of the following is not seen with ileal resections?