Biochemistry
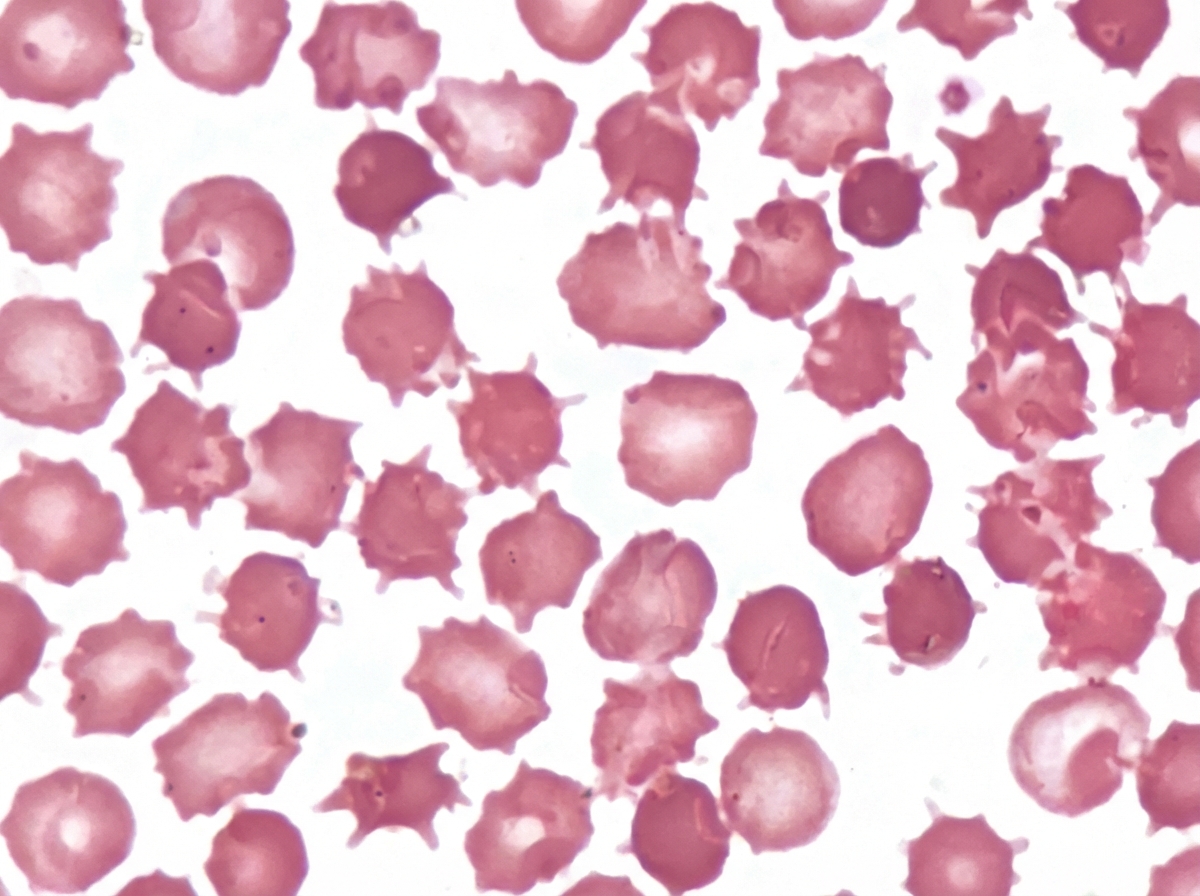
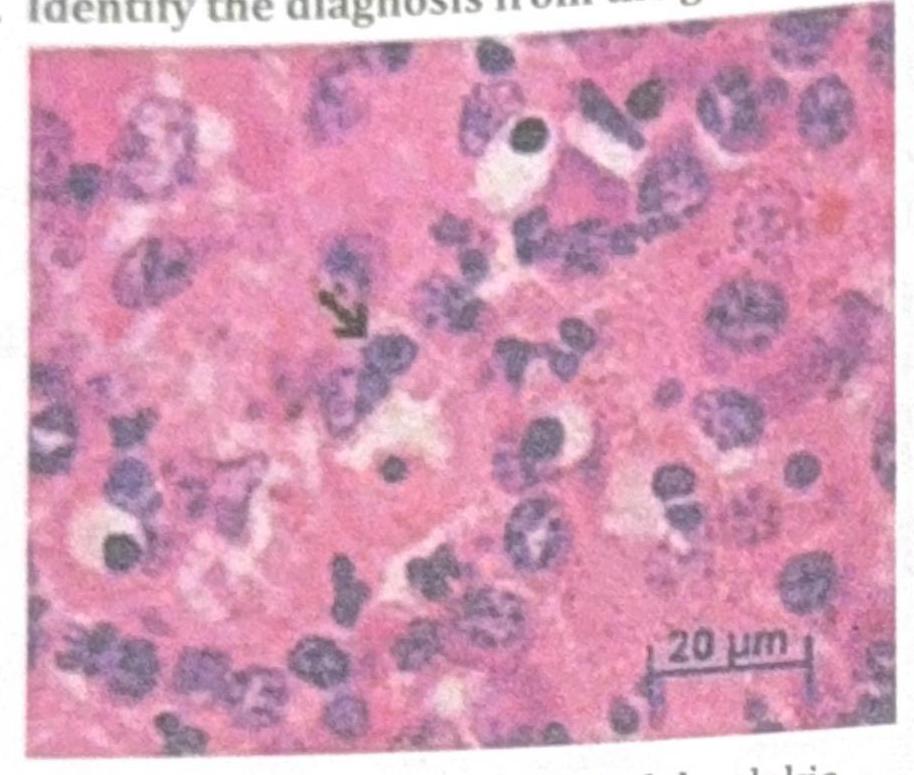
1 questionsAn adult male presented with a protruding abdomen, diarrhea, visual symptoms, and neurological manifestations. His LDL is low. Based on the peripheral smear finding shown in the image, what is the likely diagnosis?
Dermatology
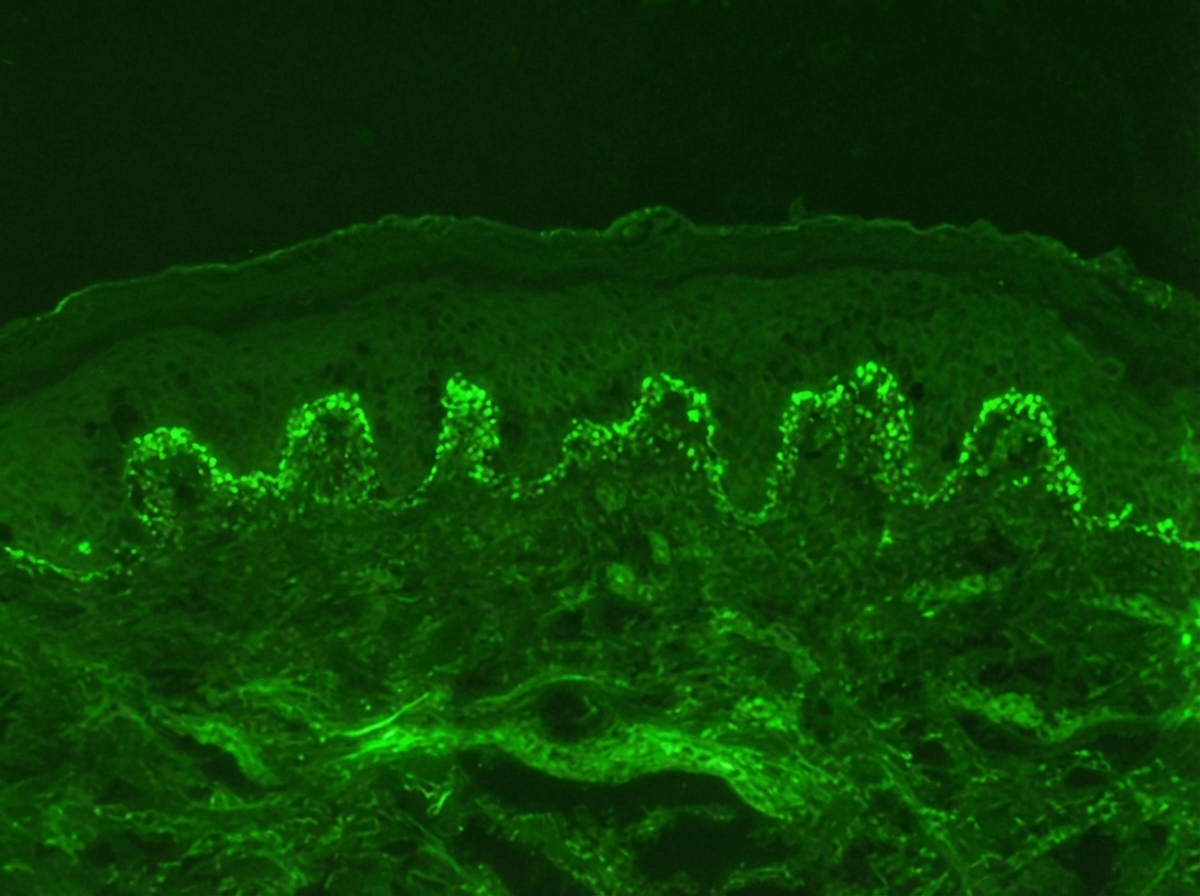
1 questionsIdentify the diagnosis based on the dermatology immunofluorescence (IF) image provided.
Internal Medicine
4 questionsWhich of the following statements is correct about Paroxysmal Nocturnal Hemoglobinuria (PNH)?
A patient presents with pulmonary hemorrhage and is P-ANCA positive. What is the most likely diagnosis?
Which of the following is typically observed in the investigation results for a patient with iron deficiency anemia (IDA)?
An adult female presents with pallor and fatigue. Blood investigations show low hemoglobin ( Hb ), low serum iron, low ferritin, low transferrin saturation, and increased total iron-binding capacity (TIBC). What is the likely diagnosis?
Pathology
4 questionsA patient presents with respiratory distress and is diagnosed with panacinar emphysema. Which of the following is deficient?
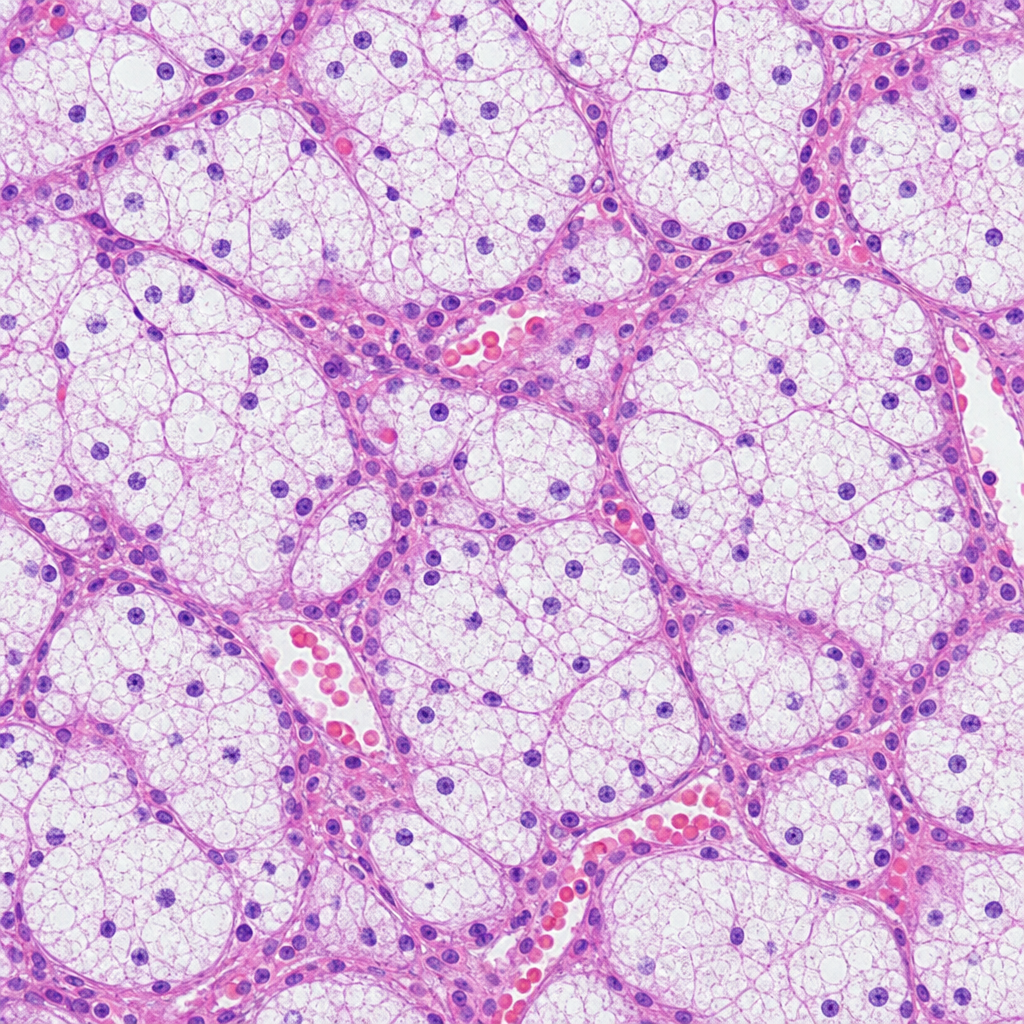
A patient presents with a renal mass leading to hematuria and flank pain. The histological image below is shown. What is the likely diagnosis?
Identify the diagnosis from the given image
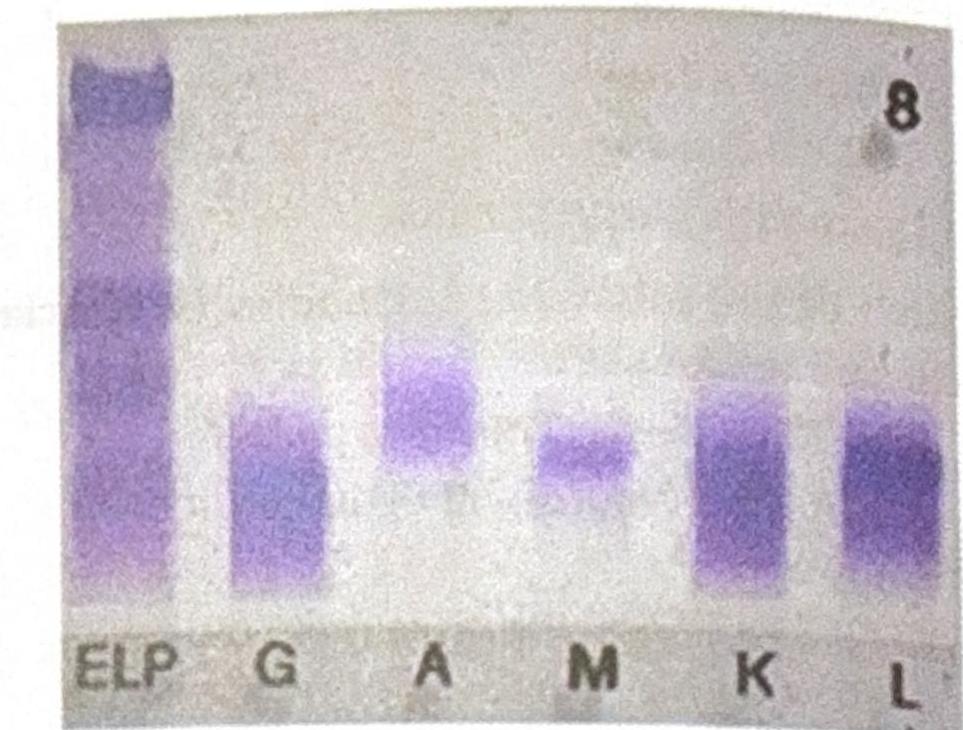
An elderly male patient presented with clinical symptoms and signs consistent with possible multiple myeloma. Electrophoresis shows an M spike, and immunofixation findings are shown below. Which of the following statements best corresponds to the findings?