Internal Medicine
1 questionsWhich of the following antibodies is associated with Celiac disease?
Microbiology
1 questionsA patient is a known case of thalassemia. Which of the following viruses would be responsible for attacking progenitor cells and causing aplastic anemia?
Pathology
7 questionsA patient has a cerebellar mass, renal tumor, and a family history of similar conditions. Which of the following mutations is most likely present in the family?
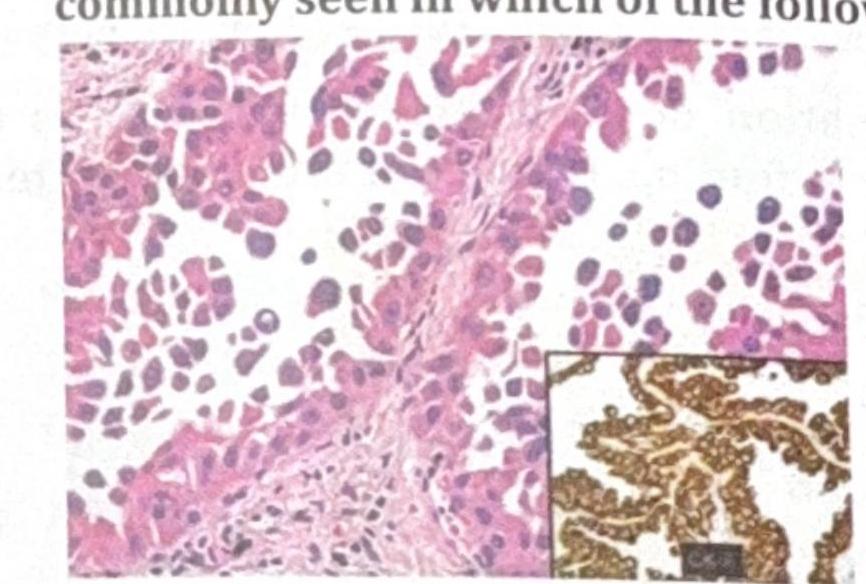
TTF-1 (Thyroid Transcription Factor-1) immunohistochemical marker is most commonly seen in which of the following?
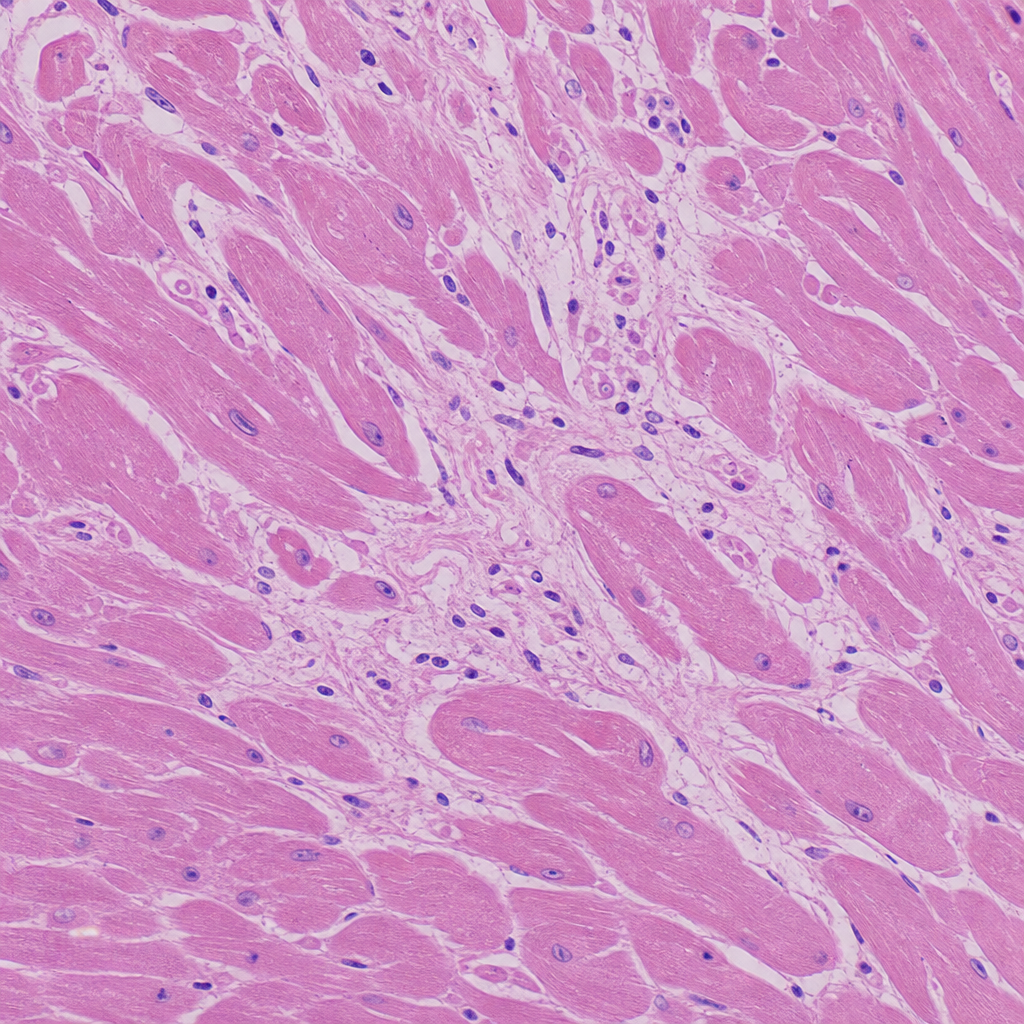
A 30-year-old football player presented to the emergency department with sudden cardiac arrest/collapse. Based on the histological image provided, what is the most likely cause of his death?
The skin biopsy shown below is most consistent with which of the following conditions? 
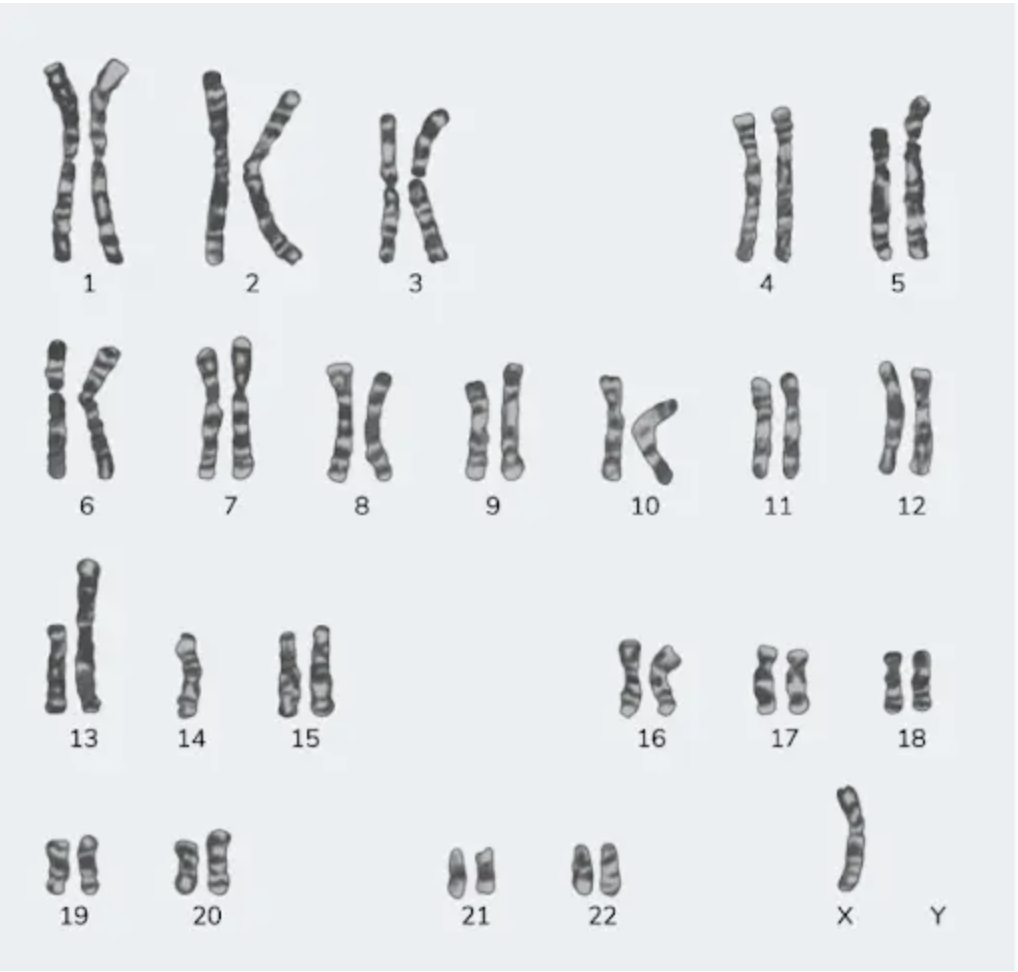
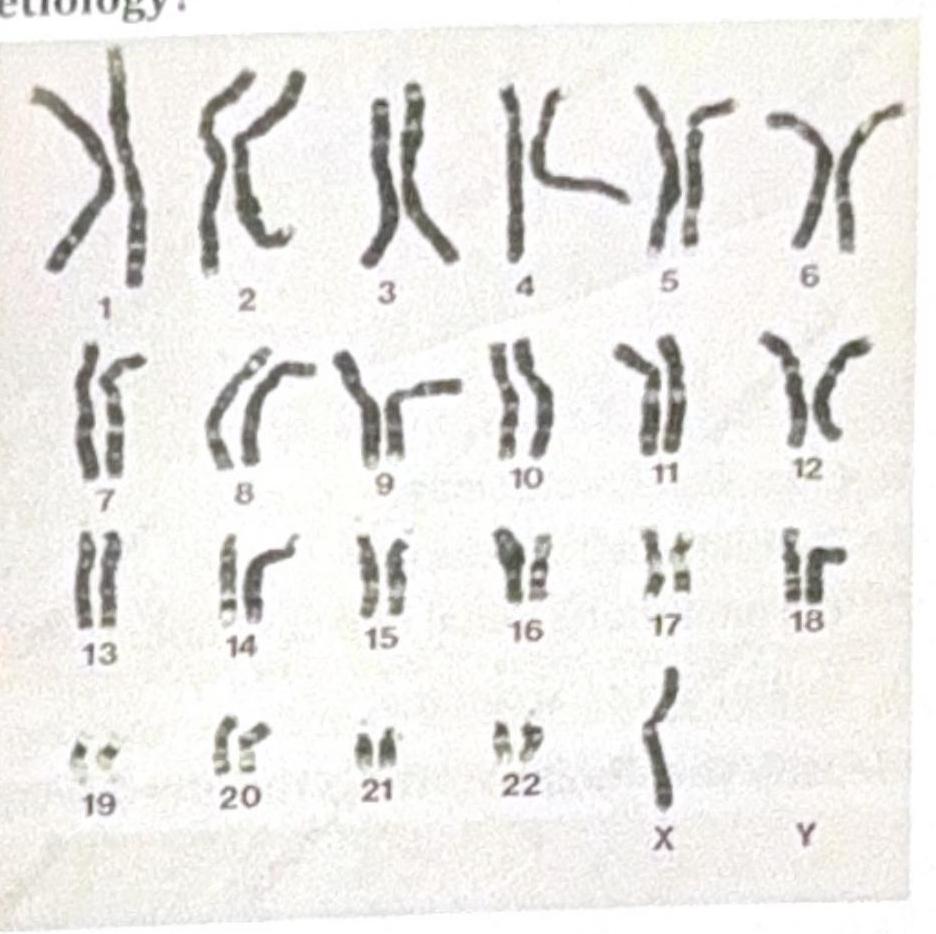
A 23-year-old female with a height of 4 feet has a karyotype as shown in the image below. Which among the following indicates the correct etiology?
The histopathology image shown is characteristic of which of the following diseases? 
A male patient is not responding to oxygen therapy and has been diagnosed with ARDS (Acute Respiratory Distress Syndrome). What is the role of IL-8 in ARDS?
Pediatrics
1 questionsA child presents with itchy lesions and diarrhea and has been advised to follow a gluten-free diet. What is the most likely etiology of this condition?