Forensic Medicine
3 questionsWhich of the following is true regarding adipocere formation?
Who orders the autopsy in the case of a Road Traffic Accident (RTA)?
Mees' lines and raindrop pigmentation on the hands are seen in which type of poisoning?
Microbiology
1 questionsThe image shows microscopic organisms. What is the most appropriate description of these organisms?

OB/GYN
2 questionsA 27 -week pregnant woman with a fetus diagnosed with congenital anomalies is considering a Medical Termination of Pregnancy (MTP). Whose presence is not required for the authorization of MTP in this case?
A USG (ultrasound) shows two babies, one of whom appears to be one month older than the other. What is the term for this condition?
Pathology
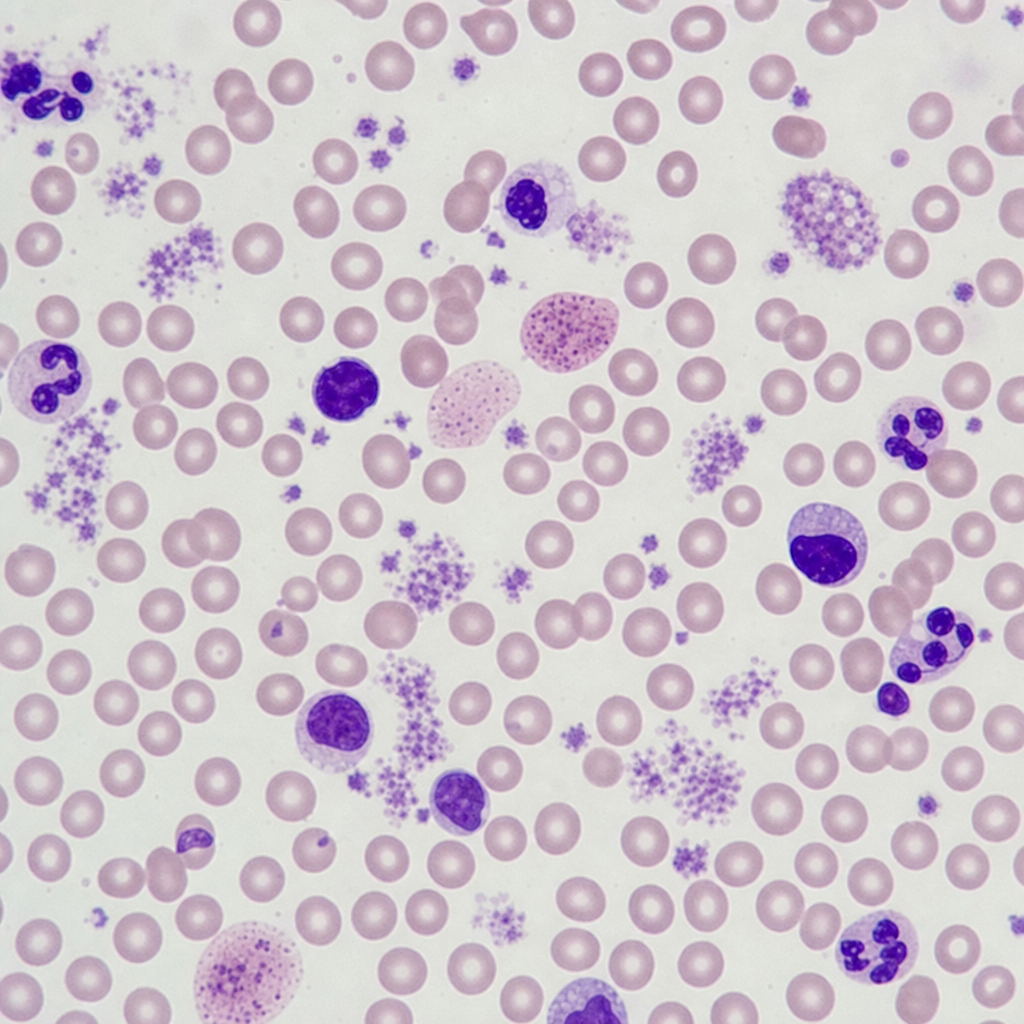
3 questionsA 34-year-old female presented with low hemoglobin, platelet count of $25,000 / \mathrm{mm}^{3}$, raised PT and APTT. The image shows a peripheral smear. Which of the following fusion genes is affected?
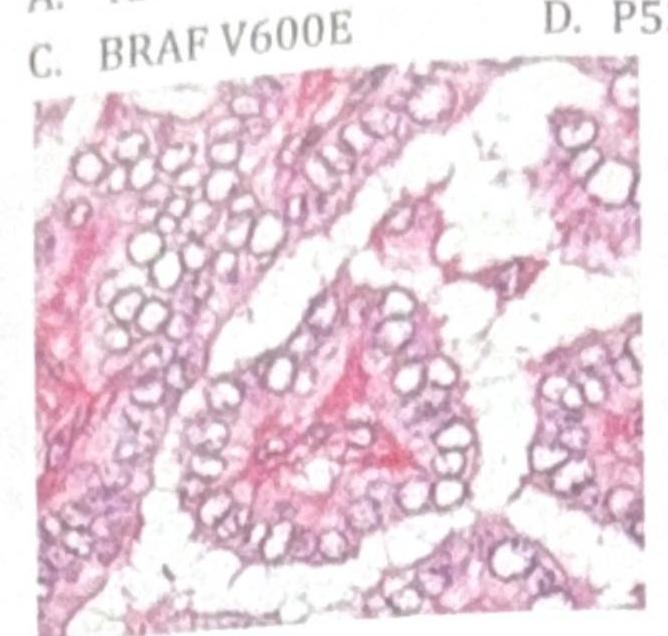
Identify the gene commonly involved in the condition shown in the image?
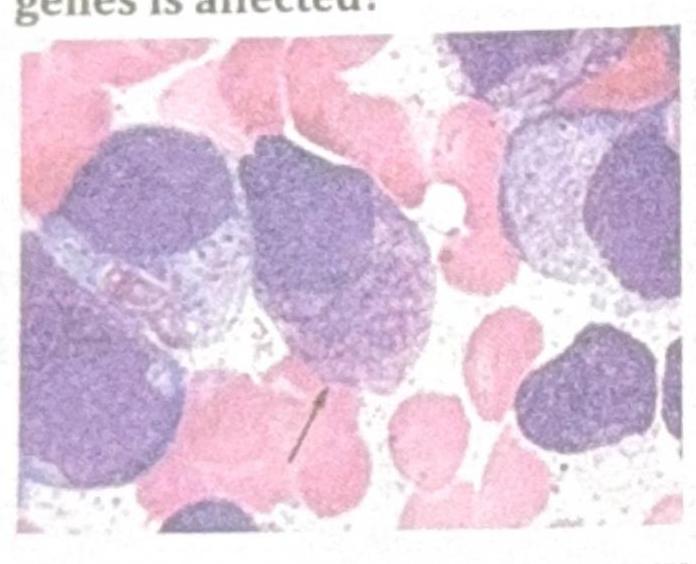
A patient presents with tingling sensation in both legs, polyuria, and weight loss. The bone marrow aspirate findings are shown in the image. What is the most likely diagnosis?
Pharmacology
1 questionsWhich of the following chelating agents is indicated in iron overdose?