Anesthesiology
1 questionsA patient with mild to moderate renal failure requires reversal of muscle relaxation induced by vecuronium. Which of the following drugs is appropriate for this purpose?
Biochemistry
2 questionsWhat is the primary function of IL-8?
Which PCR technique is best suited for identifying a syndrome with multiple causative agents?
Community Medicine
1 questionsA patient from Bihar is admitted with splenomegaly and clinical features suggestive of leishmaniasis. What is the vector responsible for transmitting this disease?
Microbiology
5 questionsA woman presents with a chronic history of fever and lower limb swelling. The microscopic image of a parasite in her blood smear is shown. Identify the pathogen responsible for her condition.

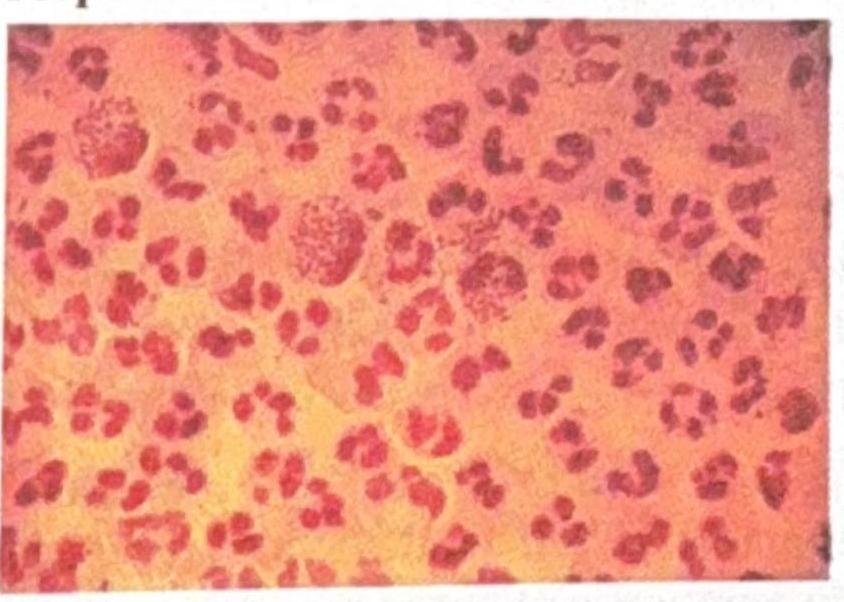
A man presents with dysuria and urethral discharge after a history of unprotected sex. The Gram stain of his discharge is shown. What is the best culture medium for isolating the organism responsible?
A young boy who used to wash his contact lenses in tap water or with unhygienic lens fluid developed keratitis. Microscopy revealed an organism with spiked or star-shaped structures. Identify the correct organism responsible.
A patient in the ICU with a central venous catheter (CVC) develops an infection. Microscopy reveals ovoid budding yeast cells. What is the most likely organism?
A farmer presents with a subcutaneous wound on his foot with discharge. Microscopy of a white granule from the wound shows Gram-positive filamentous rods. What is the most likely organism?
Pharmacology
1 questionsWhich of the following cardioselective betablockers has been shown to decrease mortality in patients with congestive heart failure?