Anatomy
4 questionsAn absent gag reflex can result from injury to which of the following nerves?
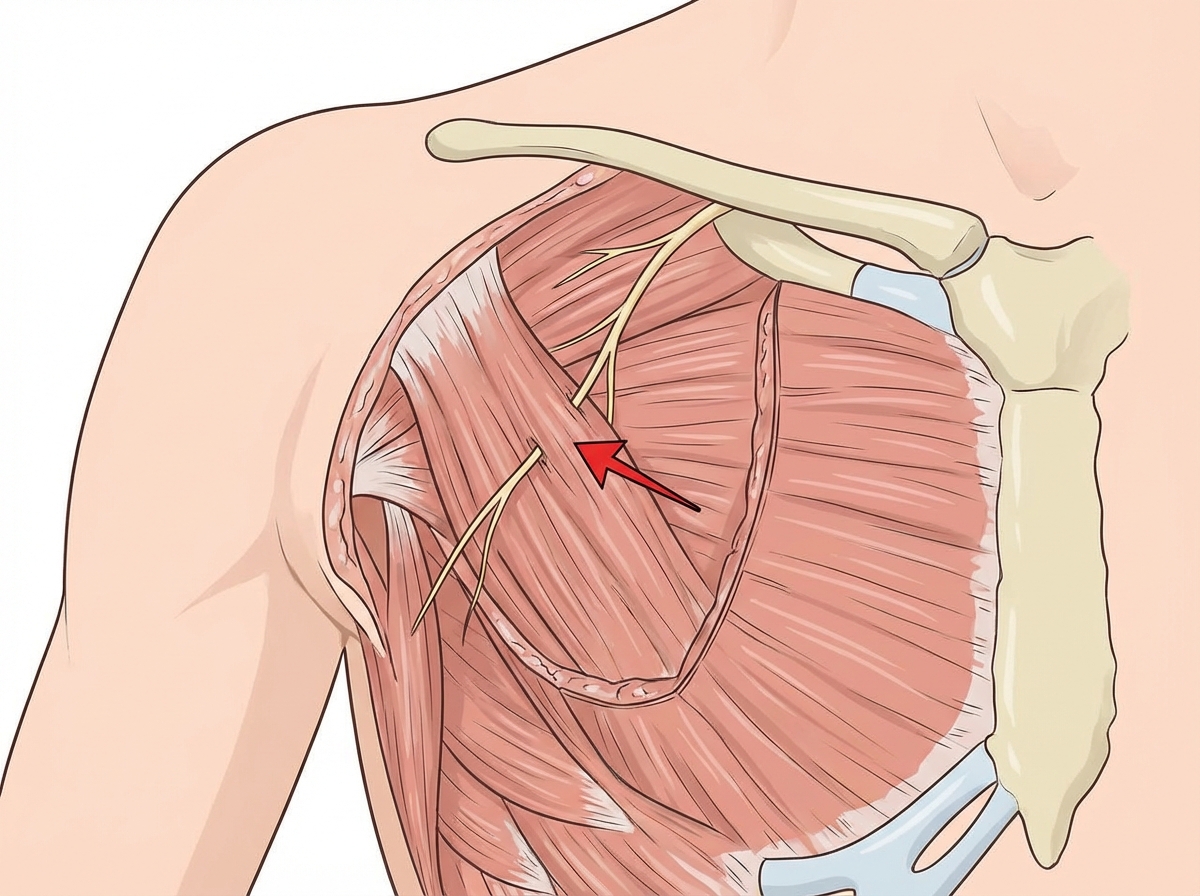
Identify the arrow marked nerve 
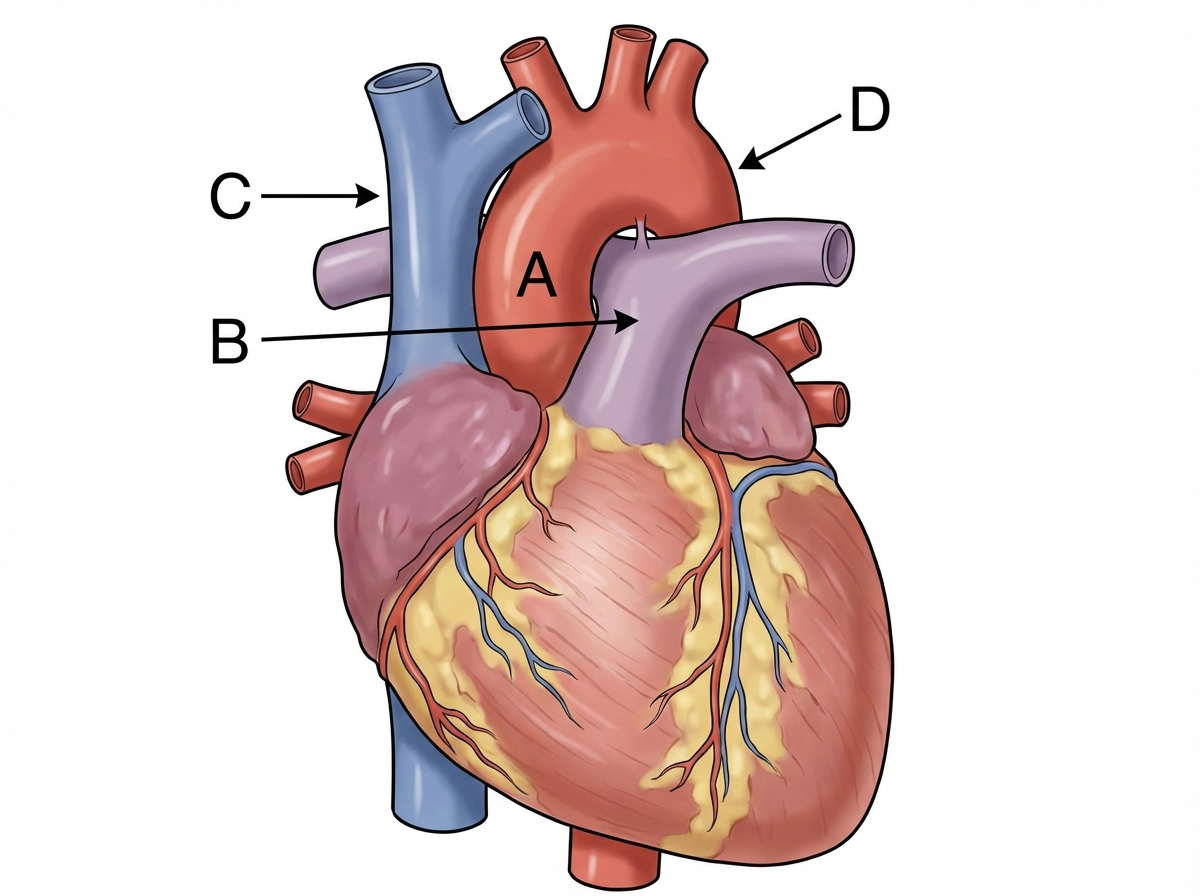
Identify the labeling correctly 
The covering of an omphalocele is derived from which of the following layers?
ENT
1 questionsA singer presents with difficulty singing at a high pitch. On examination, bowing of the vocal cord is observed on the right side. Which of the following muscles has likely been compromised?
Pediatrics
1 questionsWhat is the diagnosis based on the image shown 

Physiology
2 questionsMatch the following receptors with their correct functions: Receptors: 1. Ruffini corpuscle 2. Merkel cells 3. Pacinian corpuscle 4. Meissner's corpuscle Functions: A. Vibration B. Sustained pressure C. Stretching D. Fine touch Select the option that correctly matches each receptor (1-4) with its function (A-D).
What are the effects of a lesion in Brodmann area 22?
Surgery
2 questionsA patient presents with fecal discharge from the umbilicus. What is the most likely diagnosis?
What is the diagnosis based on the image shown?
