Anatomy
1 questionsWhich of the following nerves has the shaded cutaneous territory

Anesthesiology
1 questionsWhich IV anesthetic does not cause cardiac depression?
Internal Medicine
1 questionsA 65-year-old alcoholic is admitted to the ICU with a diagnosis of acute pancreatitis. After 48 hours, he is unconscious and has the following findings: SpO2= 60%, PO2= 60 mmHg, PCO2=50 mmHg, and HR= 120 bpm. A chest X-ray was performed and is given below. What is the diagnosis of the following condition?

Pathology
2 questionsCholesterol gallstones are made up of:-
McCallum patches/plaques are usually seen in which chamber of the heart?
Pediatrics
1 questionsWhich among the following is NOT part of the classic clinical triad of necrotizing enterocolitis?
Pharmacology
1 questionsDrug of choice for Digoxin induced Ventricular Tachycardia:
Physiology
1 questionsAll are true about Decerebrate posture except:-
Surgery
2 questionsAll of the following statements are true about Frey's Syndrome except
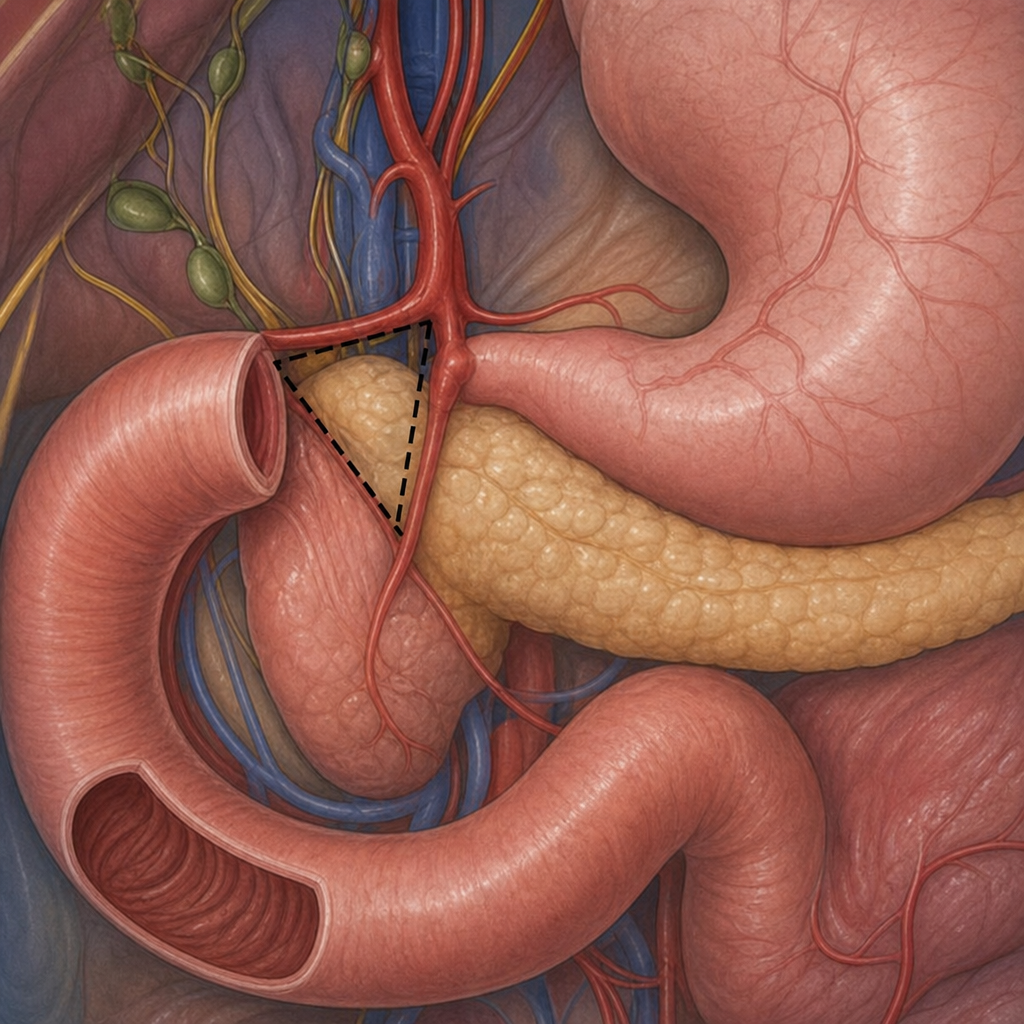
What is the name of this triangle?