Anatomy
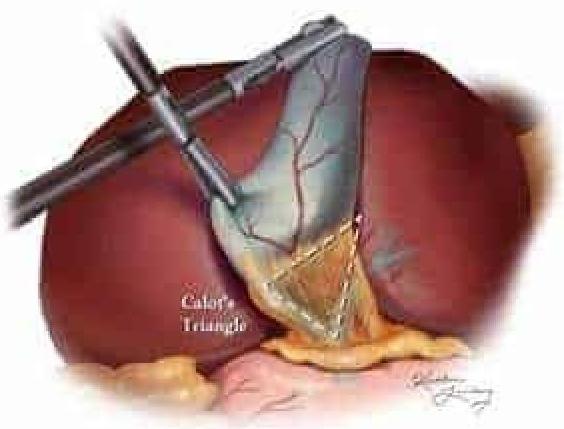
2 questionsWhich of the following structures is not a boundary of Calot's triangle shown in the given image?
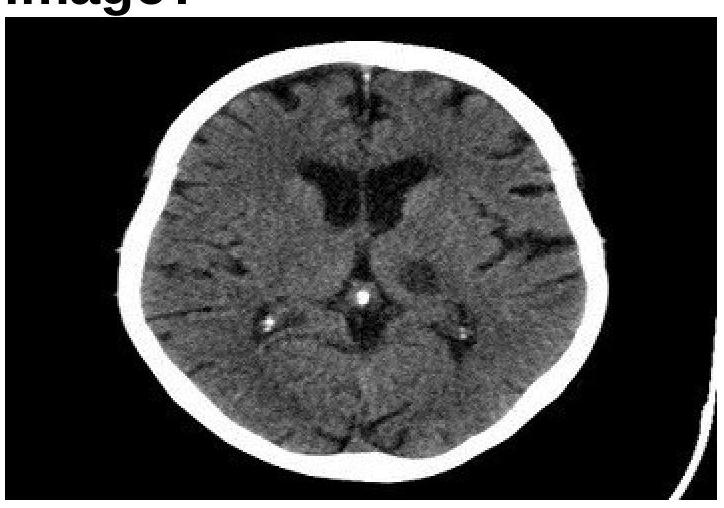
Identify the type of the fibre marked in the image of the internal capsule.

ENT
3 questionsInspiratory stridor is found in what kind of lesions:
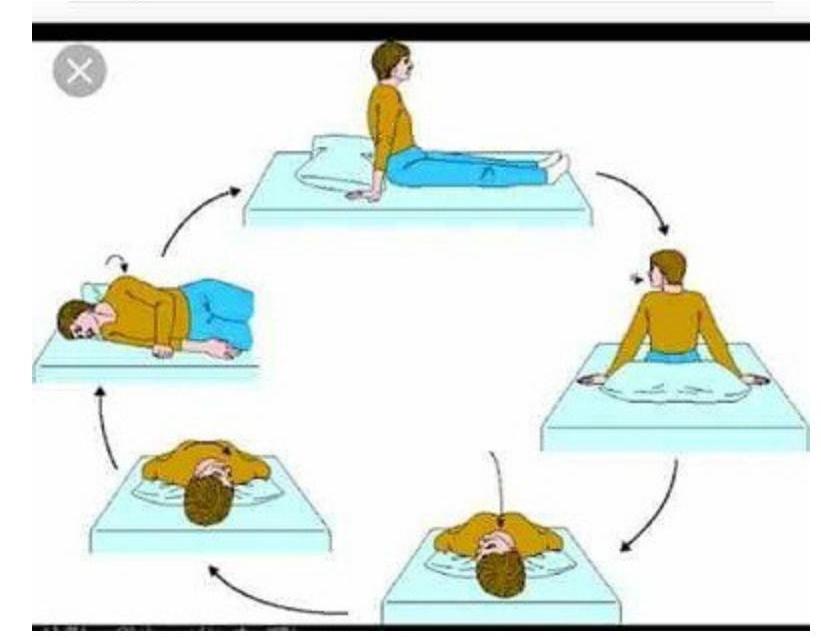
Identify the maneuver shown in the image.
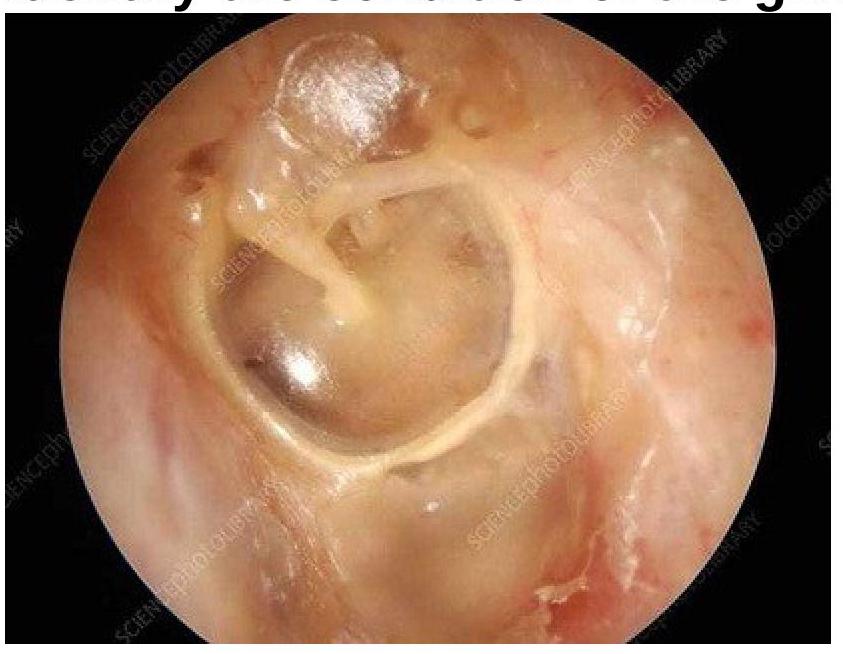
Identify the condition of the given image:
Forensic Medicine
1 questionsA patient with a history of breast cancer with brain metastases dies following a cerebral hemorrhage. According to standard death certification practices (WHO guidelines), what should be recorded as the immediate cause of death in Part I(a) of the death certificate?
Internal Medicine
2 questionsWhat are the essential major blood culture criteria for diagnosing infective endocarditis?
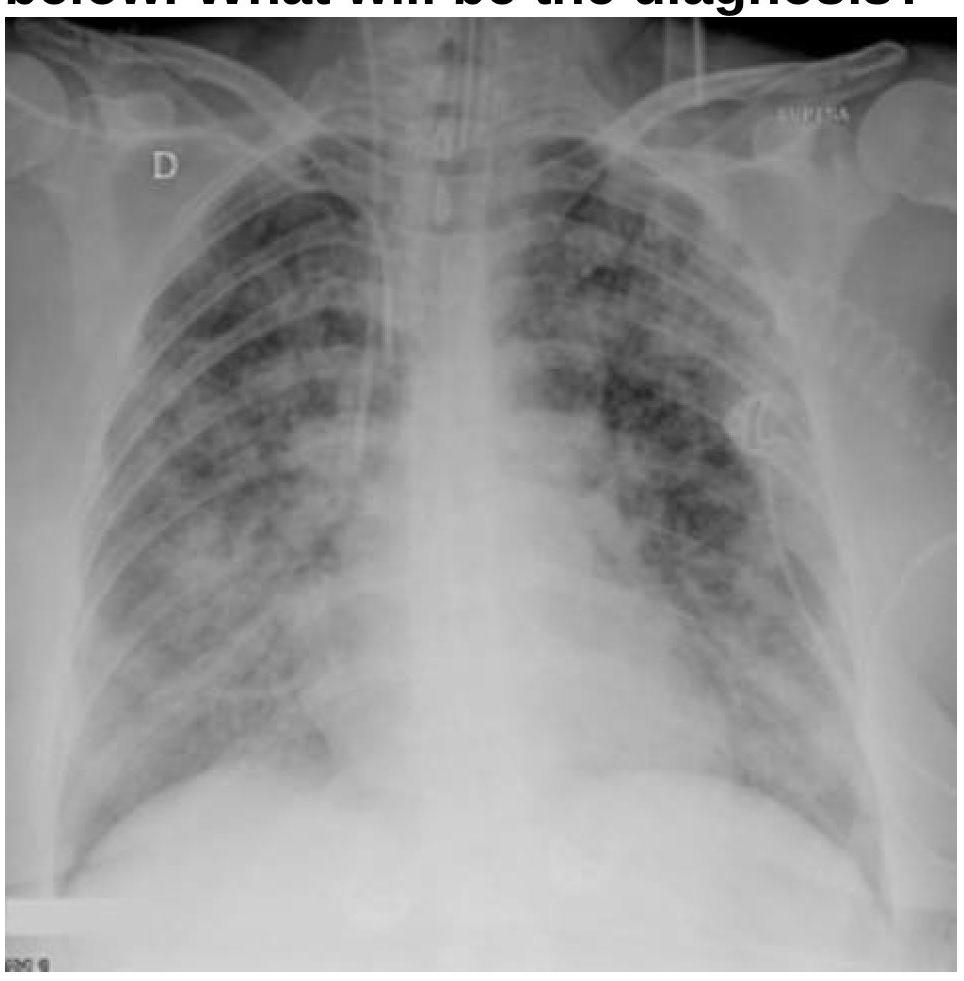
A patient with a known case of acute pancreatitis develops breathlessness and bilateral basal crepitations on day 4. What is the most likely diagnosis based on the chest radiography image?
Pediatrics
1 questionsA baby born at 34 weeks gestation weighs 3kg. Which of the following conditions is this child most likely to develop in the immediate postnatal period?
Radiology
1 questionsIdentify the condition in the image below?