All (1550)Anatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Anatomy
1 questionsQ931
Which of the following arteries does NOT contribute to Little's area?
Biochemistry
1 questionsQ931
In which condition is the Albumin to Globulin (A:G) ratio maintained?
General Medicine
1 questionsQ931
Which of the following is a complication of total parenteral nutrition?
Internal Medicine
1 questionsQ931
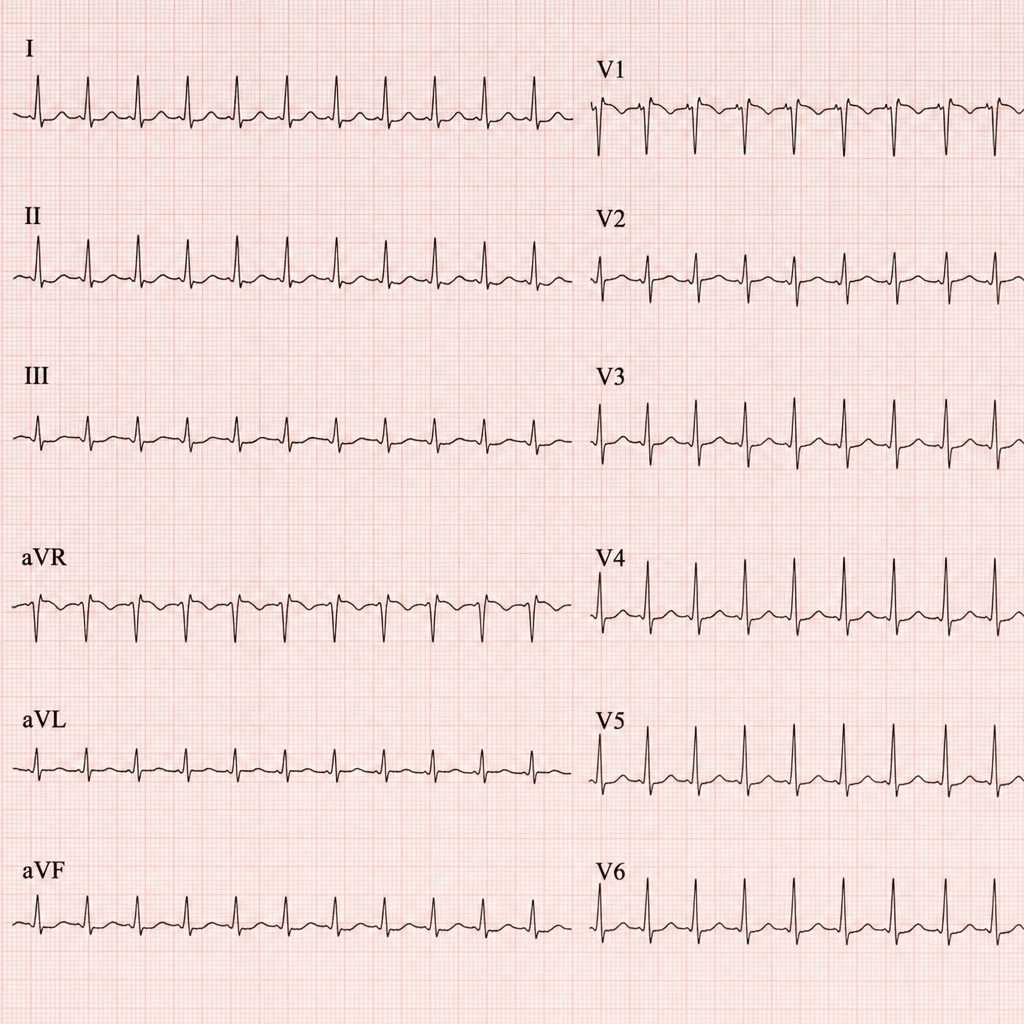
This patient came to the casualty with palpitations. His ECG has been shown below. What is your diagnosis?
Ophthalmology
3 questionsQ931
Retinitis pigmentosa is characterized by ?
Q932
Which of the following statements about the c-wave in electroretinogram (ERG) is most accurate?
Q933
Krukenberg spindles -
Pathology
1 questionsQ931
What is a watershed infarct in the brain?
Pediatrics
1 questionsQ931
At what age do the proportions of intracellular fluid (ICF) and extracellular fluid (ECF) in a child approximate those of an adult?
Pharmacology
1 questionsQ931
What is the drug of choice for the treatment of kala-azar?