Anesthesiology
2 questionsThe duration of spinal anaesthesia is based directly on:
Which of the following is used for day care surgery?
Biochemistry
1 questionsSynovial fluid contains-
ENT
1 questionsFrontal headache is due to inflammation of which sinus?
Microbiology
2 questionsMost sensitive test for detecting microfilariae?
A patient presents with suspected diphtheria. What media will be used to diagnose this condition?
Obstetrics and Gynecology
1 questionsAmsel's criteria are used for?
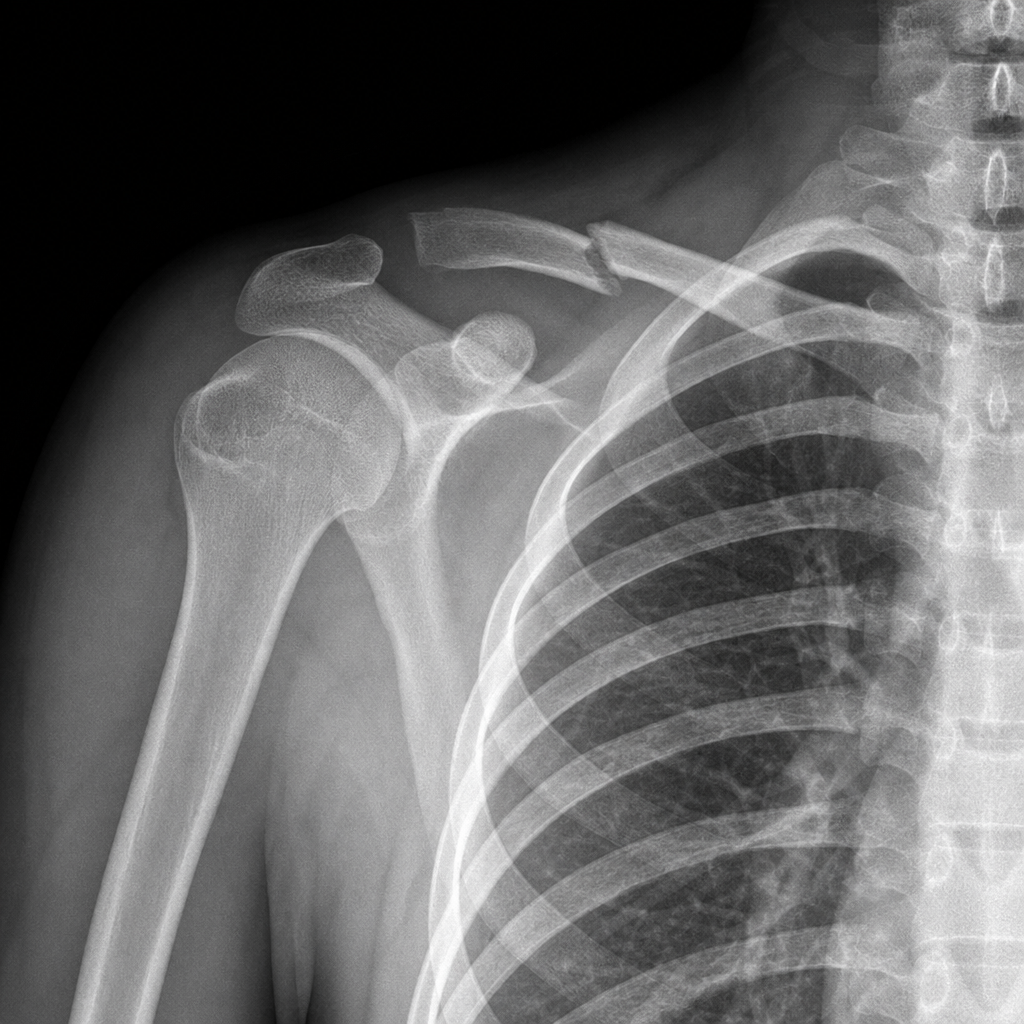
Orthopaedics
1 questionsA boy was riding bicycle, he fell down forward and injury to his shoulder was seen, which nerve injury will be seen in the condition as given in X-ray?
Pharmacology
2 questionsPraziquantel is used for the treatment of
A lady has taken medication for amoebiasis infection. She drank alcohol on the same day. She has nausea, vomiting, and dizziness. Which anti-amoebic drug could have led to interaction with alcohol to produce these symptoms?