Biochemistry
1 questionsGluconeogenesis is inhibited by?
Obstetrics and Gynecology
2 questionsA 35-year-old woman at 36 weeks of gestation presents with a history of 5 convulsions at home. Her BP is 170/100 mmHg. The diagnosis made by the doctor is eclampsia. What is the next management?
hCG is secreted by?
Ophthalmology
1 questionsA 20-year-old male complains of repeated changes in glasses prescription. This is most likely caused by:
Orthopaedics
1 questionsA 6-year-old child is suspected with supracondylar fracture of right hand, complaining of pain and swelling. X-ray of right elbow was not significant. What is the next best step in this case?
Pediatrics
1 questionsSixth disease is?
Pharmacology
3 questionsWhich of the following is the chemoprophylaxis of choice in a person who is on a journey to endemic malarial region?
Therapeutic drug monitoring is done for:
Mechanism of action of allopurinol is
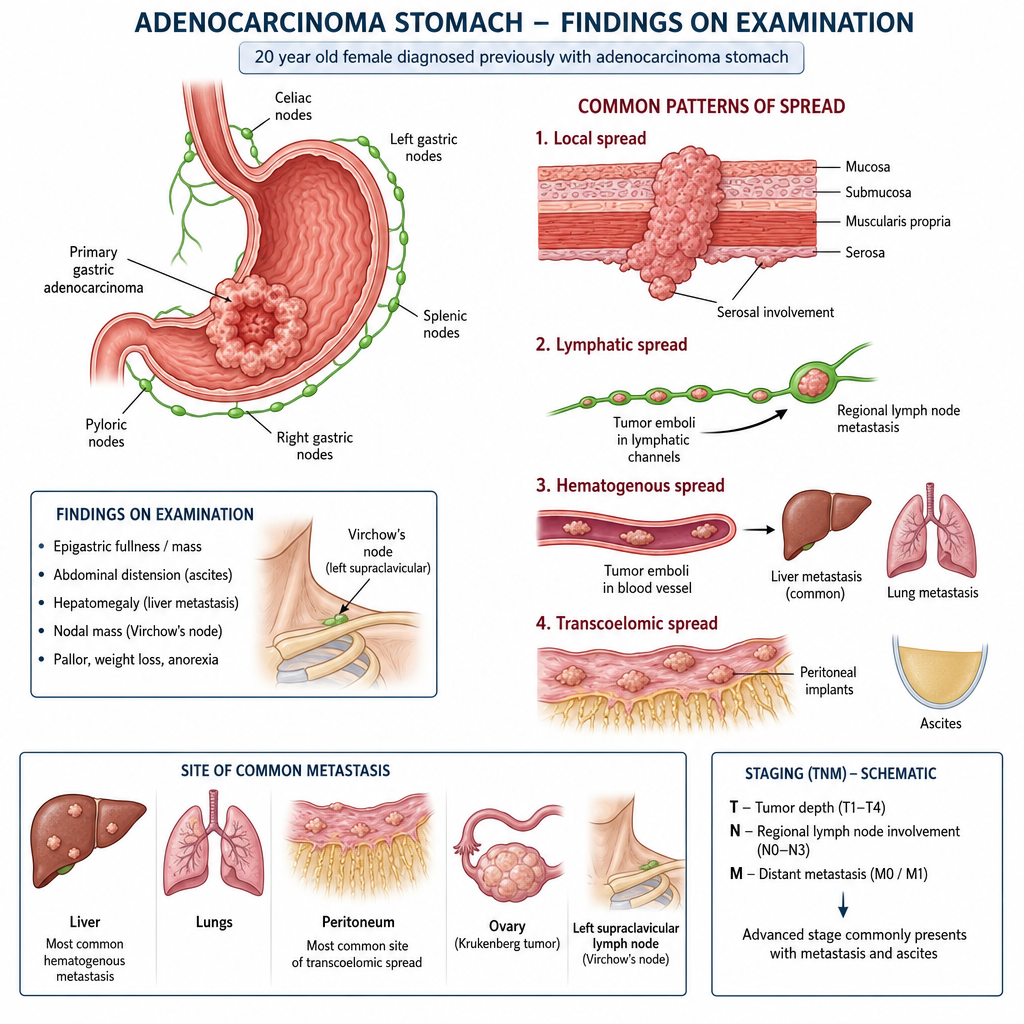
Surgery
1 questions20 yr old female diagnosed previously with adenocarcinoma stomach and on examination following is seen;