Anatomy
2 questionsProtrusion of mandible is due to which of the following muscles?
Which structure doesn't pass through the parotid gland?
Biochemistry
1 questionsType IV complex of ETC is inhibited by
Community Medicine
2 questionsIn Africa, vaccination was given in an endemic outbreak area for a specific disease but due to shortage of vaccines, mass chemoprophylaxis treatment was given to people who were not diseased. Which type of prevention is this?
Patients are categorized on the basis of chances of survival in Disaster management:
ENT
1 questionsAll the following are true about Meniere's disease except?
Forensic Medicine
1 questionsWhich of the following can be considered as grounds of divorce under matrimonial law?
Internal Medicine
1 questionsWhich of the following is seen in mitral stenosis?
Microbiology
1 questionsSmallest cestode among the following:
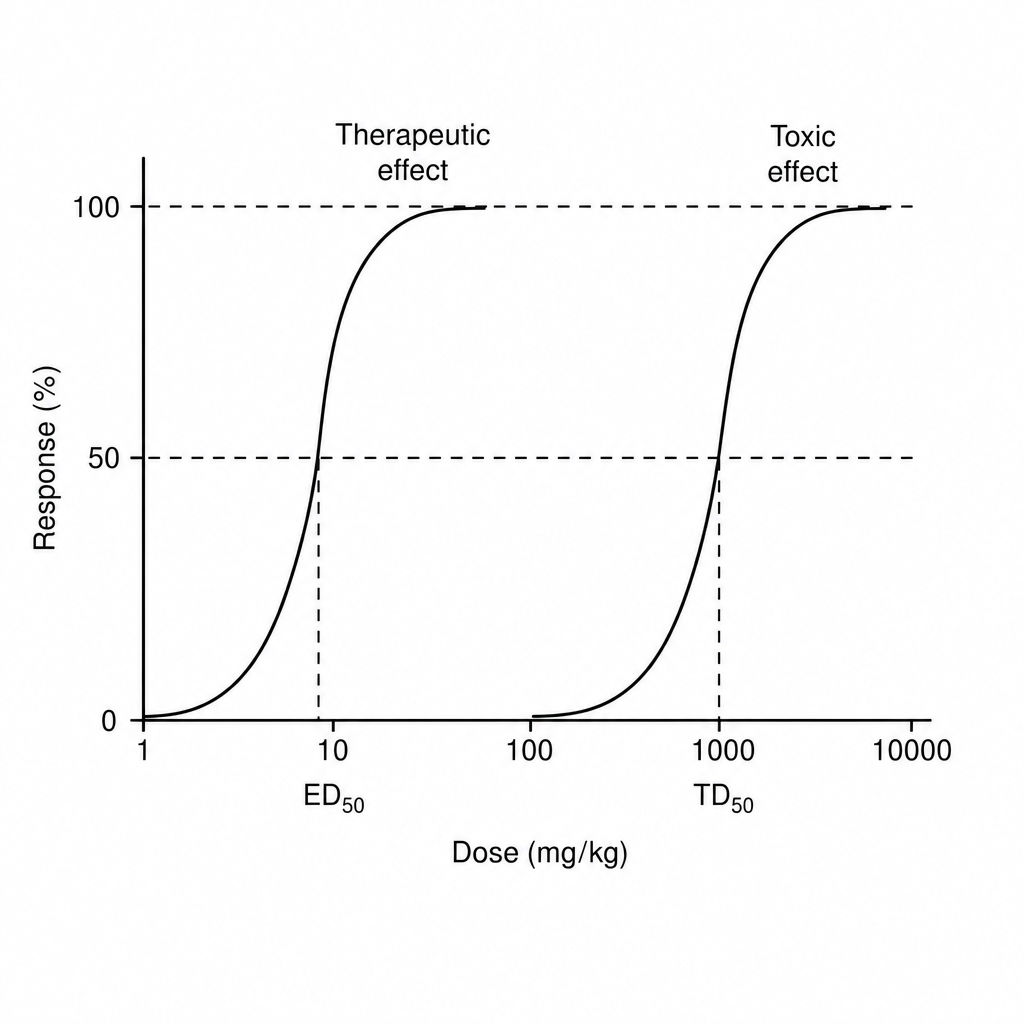
Pharmacology
1 questionsFind therapeutic index of drug from the information given below in the graph