
Bacteriology — MCQs

On this page
A patient undergoing chemotherapy develops a cough. Acid-fast stain of his sputum shows rods and slightly longer forms, with some branching; they vary in their acid-fast reaction from one area of the slide to the next. The acid-fast stain was performed by an experienced medical technologist and, when redone, showed the same variation. The growth was done aerobically. What is the most likely agent?
Agglutination with 'O' antigen of S. typhi is inhibited by which of the following?
Most of the Pseudomonas infections are based on opportunism. Which of the following is an exception?
Magnesium-ammonium phosphate stones are usually secondary to urinary tract infection with which of the following organisms?
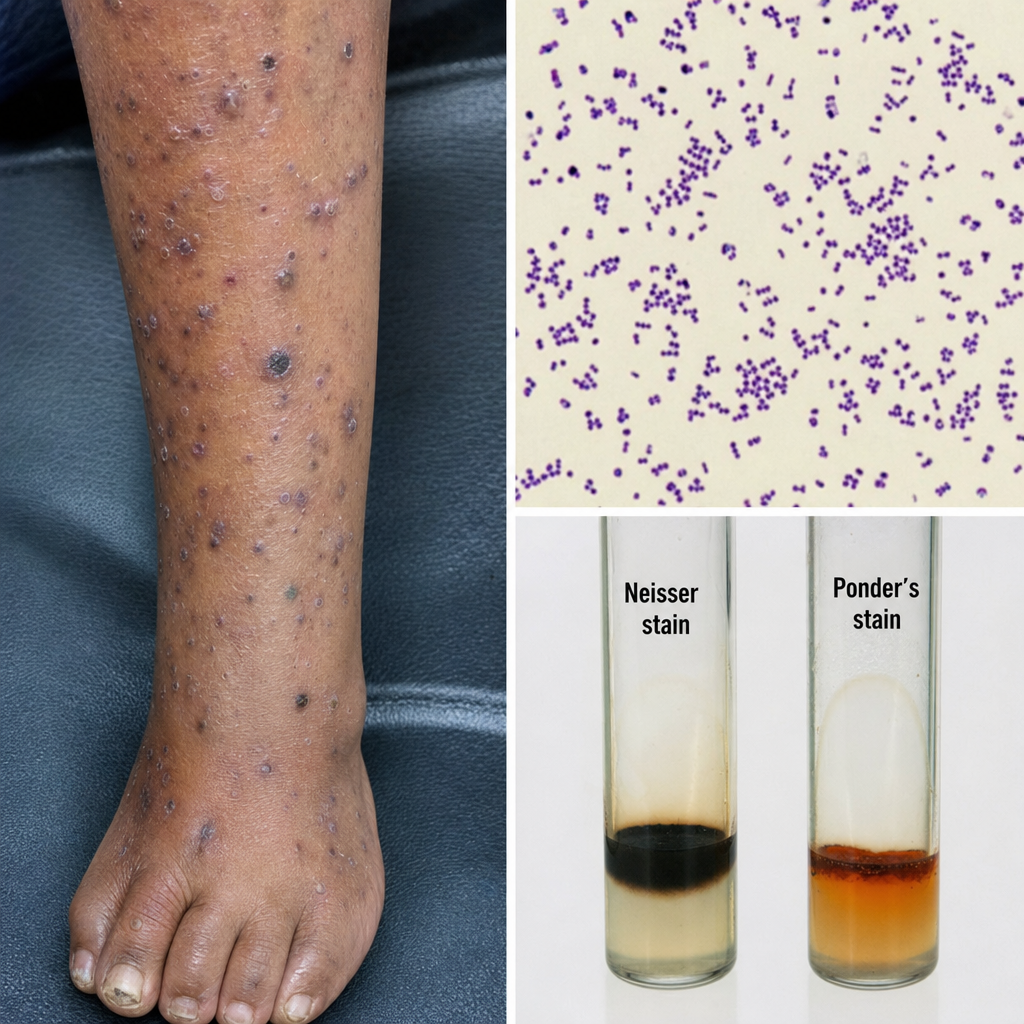
Which of the following is NOT true about the given bacteria?
What is the optimal temperature required for the isolation of Campylobacter species?
Which of the following conditions is caused by Chlamydia pneumoniae?
On a stained slide, Clostridium tetani has the appearance of a:
A 70-year-old nursing home patient developed influenza, refused the influenza vaccine, and died of an acute pneumonic attack one week after the initial influenza infection. What is the most common cause of acute post-influenza pneumonia?
A 12-year-old boy presents with pain and inflammation over the heel of his left foot and red streaks extending up the inner aspect of his leg. He recalls removing a wood splinter from the sole of his foot the previous day. What is the most likely infecting organism?
Practice by Chapter
Staphylococci
Practice Questions
Streptococci and Enterococci
Practice Questions
Neisseria and Moraxella
Practice Questions
Corynebacterium and Listeria
Practice Questions
Bacillus and Clostridium
Practice Questions
Enterobacteriaceae
Practice Questions
Vibrio, Aeromonas, and Plesiomonas
Practice Questions
Pseudomonas and Related Bacteria
Practice Questions
Haemophilus and HACEK Group
Practice Questions
Bordetella and Brucella
Practice Questions
Mycobacteria
Practice Questions
Spirochetes
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app