Q11
Which of the following statements about mesh skin grafts is not correct?
Q12
The following operative procedure can result in neurogenic voiding dysfunction except:
Q13
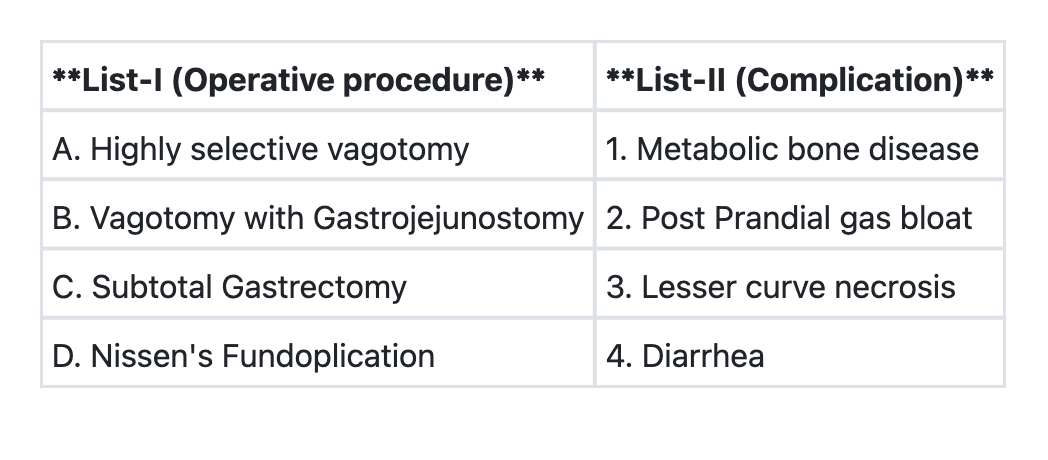
Match List-I with List-II and select the correct answer using the code given below the Lists: **List-I (Procedure)** A. Highly selective vagotomy B. Vagotomy with gastrojejunostomy C. Subtotal gastrectomy D. Nissen's fundoplication **List-II (Complication)** 1. Metabolic bone disease 2. Post-prandial gas bloat 3. Lesser curve necrosis 4. Diarrhea **Code:**
Q14
Optimum age for surgery for a child with cleft lip is:
Q15
An electrical contact burn is considered to be:
Q16
A 52 year old male patient comes with history of rectal bleeding, alteration in bowel habits and tenesmus. The ideal investigation would be:
Q17
What is the treatment of choice in a patient with Crohn’s disease, where inflamed appendix was found on exploration?
Q18
The following are features of hypovolemic shock except:
Q19
A 45 year old man sustains trauma in a road traffic accident and develops engorgement of neck veins, pallor, rapid pulse rate, and chest pain. What is the most likely diagnosis?
Q20
Which one of the following statements is not correct regarding trichobezoar ( hair balls)?