All (113)Anatomy (3)Community Medicine (31)ENT (1)Forensic Medicine (1)Internal Medicine (5)Microbiology (1)Obstetrics and Gynecology (30)Ophthalmology (1)Orthopaedics (2)Pathology (3)Pediatrics (4)Physiology (1)Psychiatry (1)Radiology (1)Surgery (28)
Q71
Face to pubes delivery occurs in which of the foetal position?
Q72
The peak level of human chorionic gonadotropin in normal pregnancy occurs between:
Q73
The second most common site for endometriosis after the ovary is:
Q74
A patient who just delivered at home presents with a third degree perineal tear. You will do the repair:
Q75
The gestational sac is first visible on transvaginal USG by:
Q76
A 30-year-old housewife reports with 6 months amenorrhea. Her serum LH and FSH are high with low estradiol levels. What is the most likely cause of amenorrhea in this context?
Q77
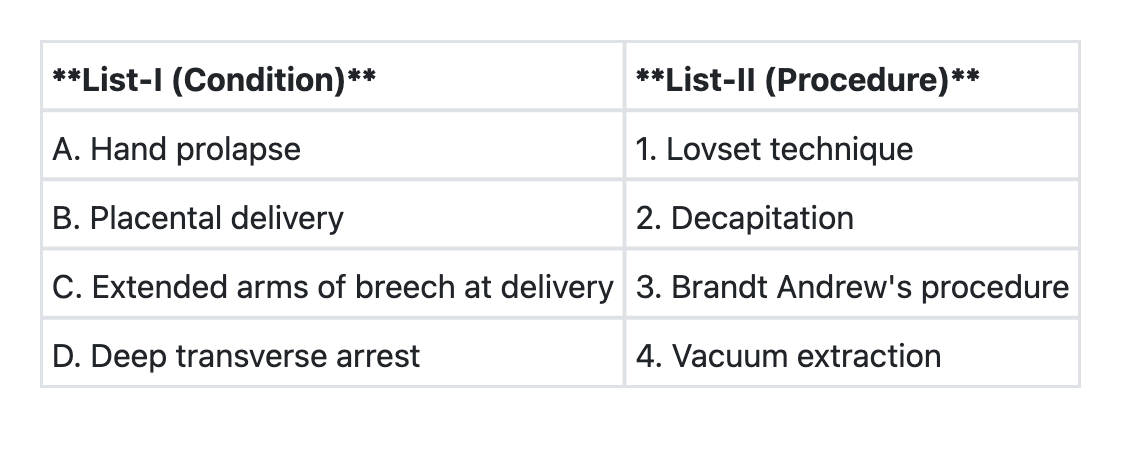
Match List-I with List-II and select the correct answer using the code given below the Lists: