All (113)Anatomy (3)Community Medicine (31)ENT (1)Forensic Medicine (1)Internal Medicine (5)Microbiology (1)Obstetrics and Gynecology (30)Ophthalmology (1)Orthopaedics (2)Pathology (3)Pediatrics (4)Physiology (1)Psychiatry (1)Radiology (1)Surgery (28)
Q31
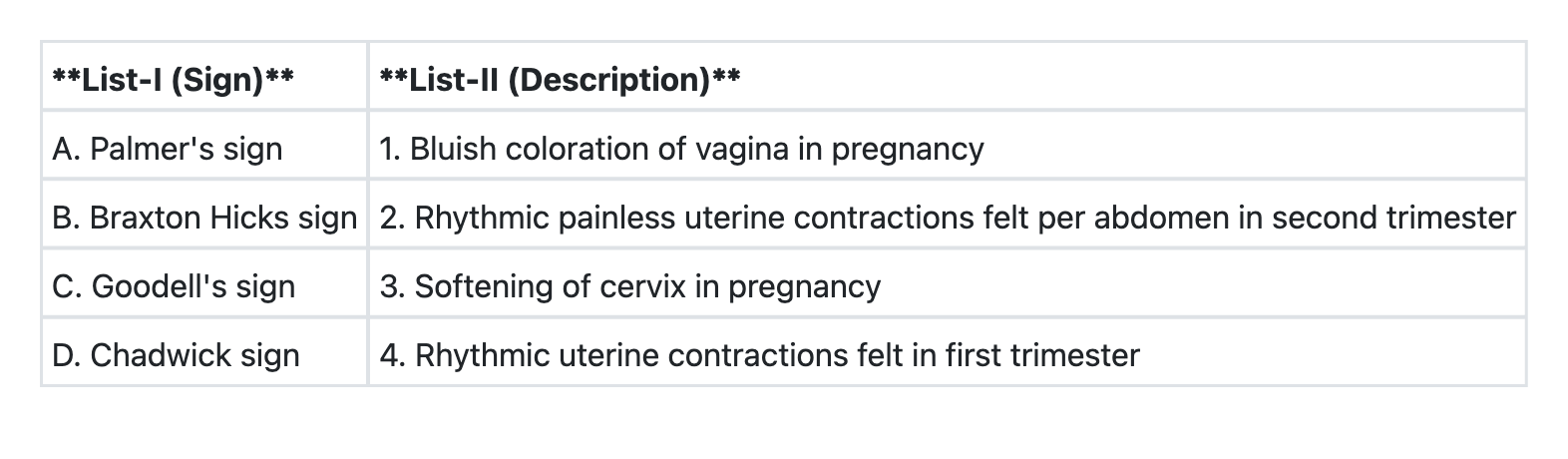
Match List-I with List-II and select the correct answer using the code given below the Lists: