All (113)Anatomy (3)Community Medicine (31)ENT (1)Forensic Medicine (1)Internal Medicine (5)Microbiology (1)Obstetrics and Gynecology (30)Ophthalmology (1)Orthopaedics (2)Pathology (3)Pediatrics (4)Physiology (1)Psychiatry (1)Radiology (1)Surgery (28)
Q91
What is the most important test to assess the prevalence of tuberculosis infection in a community?
Q92
In a normal curve, the area between one standard deviation on either side of the mean will include:
Q93
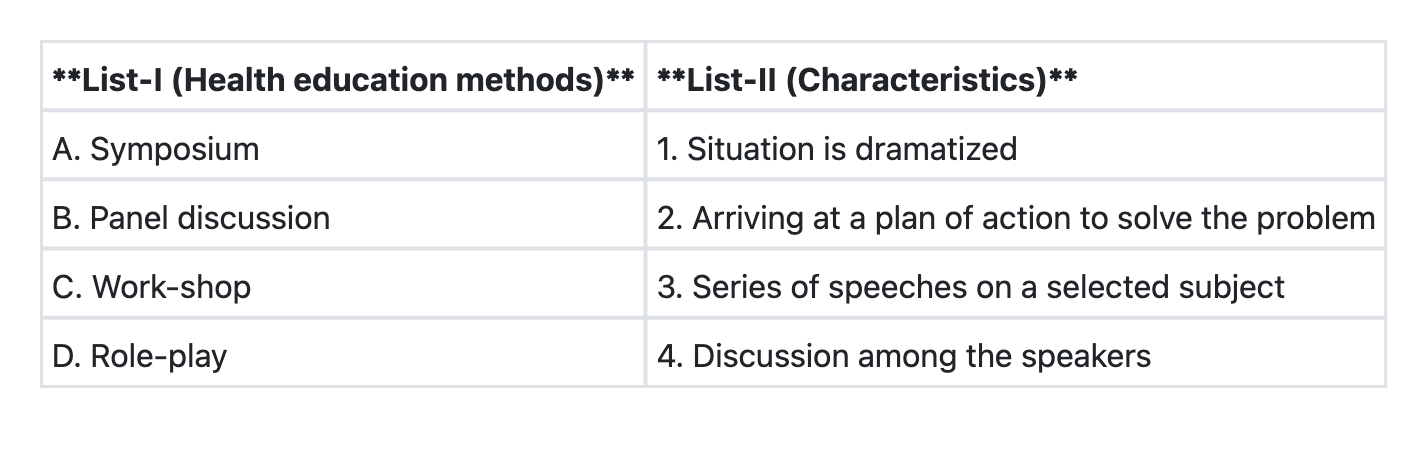
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q94
Which of the following insecticides is not used as a larvicide?
Q95
An outbreak of Viral Hepatitis was reported from a town between June and August of a particular year. 60% of cases occurred in July. Exposure of the community to infection is from:
Q96
Which one of the following indicators is not included in Millennium Development Goals?
Q97
Severity of a disease is measured by:
Q98
‘Spot map’ in epidemiological studies refer to variation in the distribution of a disease at: