During Pomeroy’s method of female sterilization, which portion of tube is ligated?
Which one of the following causes the greatest risk of ectopic pregnancy?
Face to pubes delivery occurs in which of the foetal position?
The peak level of human chorionic gonadotropin in normal pregnancy occurs between:
The second most common site for endometriosis after the ovary is:
A patient who just delivered at home presents with a third degree perineal tear. You will do the repair:
The gestational sac is first visible on transvaginal USG by:
A 30-year-old housewife reports with 6 months amenorrhea. Her serum LH and FSH are high with low estradiol levels. What is the most likely cause of amenorrhea in this context?
The Pearl index of contraceptive failure is expressed as a rate per
Match List-I with List-II and select the correct answer using the code given below the Lists:
UPSC-CMS 2014 - Obstetrics and Gynecology UPSC-CMS Practice Questions and MCQs
Question 21: During Pomeroy’s method of female sterilization, which portion of tube is ligated?
- A. Isthmo-ampullary (Correct Answer)
- B. Cornual
- C. Ampullary
- D. Isthmus
Explanation: ***Isthmo-ampullary*** - In **Pomeroy's method** of female sterilization, a loop of fallopian tube is picked up at the **isthmo-ampullary junction** (junction of middle and outer third of the tube). - This mid-portion of the tube is elevated into a knuckle, ligated at its base with absorbable suture, and the loop above the ligature is excised. - The **isthmo-ampullary junction** is the classic site described in standard texts for Pomeroy's technique, as it provides adequate length for creating a loop while maintaining sufficient distance from the uterine cornua. *Isthmus* - While the isthmus may be partially involved in the loop, **Pomeroy's method specifically targets the isthmo-ampullary junction**, not the pure isthmic segment. - Ligation of the isthmus alone (too close to the uterus) would not be the standard Pomeroy's technique and could increase risk of complications. *Cornual* - The **cornual portion** refers to the interstitial part of the fallopian tube located within the uterine wall. - This segment is not targeted in Pomeroy's method due to increased risk of uterine injury and bleeding. - Cornual resection is a different surgical approach used in other sterilization techniques. *Ampullary* - The **ampulla** is the wider, lateral portion of the fallopian tube where fertilization typically occurs. - While the ampulla may form part of the loop in Pomeroy's method, the **ligation point** is specifically at the isthmo-ampullary junction, not in the pure ampullary segment. - Ligation too far laterally in the ampulla would not be standard Pomeroy's technique.
Question 22: Which one of the following causes the greatest risk of ectopic pregnancy?
- A. Previous ectopic pregnancy (Correct Answer)
- B. Intrauterine contraceptive devices use
- C. Previous normal delivery
- D. Previous medical termination of pregnancy
Explanation: ***Previous ectopic pregnancy*** - A history of prior ectopic pregnancy significantly increases the risk of a **recurrent ectopic pregnancy** due to potential **tubal damage** from the previous event. - This is considered the **highest risk factor** among the choices provided because it indicates a pre-existing vulnerability in the reproductive system. *Intrauterine contraceptive devices use* - While IUDs do not cause ectopic pregnancies, they **prevent intrauterine pregnancies** more effectively than ectopic ones, leading to a higher proportion of pregnancies being ectopic if conception occurs. - The absolute risk of an ectopic pregnancy with an IUD in place is still **lower than in women not using contraception** but the ratio of ectopic to intrauterine pregnancies is higher. *Previous normal delivery* - A history of previous normal delivery is generally **protective against ectopic pregnancy**, as it suggests healthy tubal function and uterine environment. - This factor has **no association** with an increased risk of ectopic pregnancy. *Previous medical termination of pregnancy* - There is generally **no significant increased risk** of ectopic pregnancy associated with a single medical termination of pregnancy, especially when performed early in gestation. - Repeated or complicated terminations, especially surgical, *could* theoretically increase risk due to **tubal damage or inflammation**, but medical termination typically carries little to no added risk.
Question 23: Face to pubes delivery occurs in which of the foetal position?
- A. Occipito-sacral (Correct Answer)
- B. Brow presentation
- C. Mentoanterior
- D. Mentoposterior
Explanation: ***Occipito-sacral (Occipito-posterior)*** - **"Face to pubes" delivery** is the classic mechanism in **persistent occipito-posterior (OP)** positions where the occiput is directed toward the maternal sacrum. - In this position, the fetal head delivers with **maximum extension**, and the **face passes under the pubic symphysis** (hence "face to pubes"). - The occiput sweeps over the perineum posteriorly, leading to increased perineal trauma and potential for third/fourth-degree tears. - This delivery mechanism is associated with **prolonged labor, increased back pain**, and higher rates of operative delivery. *Mentoanterior* - In **mentoanterior (MA)** face presentation, the fetal chin is anterior, and delivery occurs by **flexion after the chin passes under the symphysis**. - The mechanism involves the chin sweeping the perineum, NOT "face to pubes" delivery. - While mentoanterior can deliver vaginally, the delivery mechanism is distinctly different from occipito-posterior positions. *Brow presentation* - In **brow presentation**, the head is partially extended with the **frontal bone and anterior fontanelle presenting**. - This presents the **largest diameter (mento-vertical ~13.5 cm)** to the pelvis, making vaginal delivery virtually impossible. - Almost always requires **cesarean section** for safe delivery. *Mentoposterior* - In **mentoposterior (MP)** face presentation, the fetal chin is directed posteriorly toward the maternal sacrum. - This position **cannot deliver vaginally** as further extension of the already extended head is impossible. - Requires **rotation to mentoanterior** or cesarean section for delivery.
Question 24: The peak level of human chorionic gonadotropin in normal pregnancy occurs between:
- A. 30 to 40 days after pregnancy
- B. 100 to 120 days after pregnancy
- C. 10 to 12 days after pregnancy
- D. 60 to 70 days after pregnancy (Correct Answer)
Explanation: ***60 to 70 days after pregnancy*** - Peak **hCG levels** in normal singleton pregnancies are typically observed between **9-10 weeks of gestation**, which corresponds to approximately **63-70 days after the last menstrual period (LMP)** or fertilization. - This period marks the highest physiological levels of hCG, crucial for maintaining the **corpus luteum** and early pregnancy. *30 to 40 days after pregnancy* - At this stage (approximately 4-5 weeks gestation), hCG levels are **rising rapidly** but have not yet reached their peak. - While detectable and increasing, the concentration of hCG is significantly lower than what is observed at 9-10 weeks. *100 to 120 days after pregnancy* - By this time (approximately 14-17 weeks gestation), **hCG levels have already peaked** and are typically declining to a lower, somewhat stable plateau for the remainder of the pregnancy. - This period is well past the peak hCG concentration. *10 to 12 days after pregnancy* - This period roughly corresponds to the time of **implantation** and the very early stages of hCG production, making levels **relatively low** but detectable. - HCG levels are just beginning their rapid ascent following implantation and are far from their peak concentration.
Question 25: The second most common site for endometriosis after the ovary is:
- A. Round ligaments
- B. Fallopian tubes
- C. Outer surface of uterus
- D. Peritoneum of the pouch of Douglas (Correct Answer)
Explanation: ***Peritoneum of the pouch of Douglas*** - The **pouch of Douglas** (rectouterine pouch) is the most common site for endometriosis after the ovaries, where endometrial tissue deposits frequently occur. - Due to its dependent position in the pelvis, **shed endometrial cells** from retrograde menstruation are thought to accumulate here. *Round ligaments* - While endometriosis can occur in the round ligaments, it is far **less common** than in the cul-de-sac or on the ovaries. - Endometriotic lesions in this location might mimic other conditions, making diagnosis challenging. *Fallopian tubes* - Endometriosis can affect the fallopian tubes, leading to conditions like **hydrosalpinx** or adhesion formation, but it is not the second most common site. - The tubes are more frequently involved by **pelvic inflammatory disease** or ectopic pregnancy. *Outer surface of uterus* - Endometriosis on the outer surface of the uterus (serosa) is possible, but **less common** than in the ovaries or the pouch of Douglas. - Lesions here can contribute to **adhesions** between the uterus and adjacent structures.
Question 26: A patient who just delivered at home presents with a third degree perineal tear. You will do the repair:
- A. after 24 hours.
- B. after 6 weeks
- C. immediately (Correct Answer)
- D. after 3 months
Explanation: ***immediately*** - Repair of a **third-degree perineal tear** should be done **immediately** after diagnosis to minimize complications like infection, pain, and long-term functional issues. - Prompt repair helps to restore **anatomical integrity** and improve outcomes for continence and discomfort. *after 24 hours.* - Delaying the repair by 24 hours increases the risk of **infection**, **edema**, and further tissue damage, making the repair more difficult and less successful. - This delay could also lead to increased **blood loss** and patient discomfort. *after 6 weeks* - Waiting 6 weeks would allow for scar tissue formation and potential infection, making a primary repair much more challenging and possibly requiring a more complex secondary repair. - This delay would significantly increase the risk of **fecal incontinence** and other long-term complications. *after 3 months* - A three-month delay is inappropriate for a fresh perineal tear as it guarantees significant **scarring**, **fibrosis**, and high risk of **infection**. - By this time, the tear would likely have healed by secondary intention, resulting in poor anatomical and functional outcomes, often necessitating a more complicated and less effective **secondary repair**.
Question 27: The gestational sac is first visible on transvaginal USG by:
- A. 49 days
- B. 30 days
- C. 42 days
- D. 35 days (Correct Answer)
Explanation: ***35 days*** - A **gestational sac** can first be reliably visualized via **transvaginal ultrasonography** at approximately **35 days** after the last menstrual period (around **5 weeks gestational age**). - At this stage, it appears as a small, anechoic (fluid-filled) structure within the **endometrial cavity**, indicating an early intrauterine pregnancy. - This corresponds to a **β-hCG level** of approximately **1000-2000 mIU/mL**, which is the discriminatory zone for transvaginal ultrasound. *30 days* - At **30 days** (approximately 4 weeks + 2 days gestational age), the gestational sac is typically **too small** to be consistently visualized even with transvaginal ultrasound. - While some early sacs may be detected, **30 days** is generally considered **too early** for reliable detection in most cases. - Detection at this stage would be inconsistent and not the standard timeframe cited in obstetric practice. *42 days* - By **42 days** (6 weeks gestational age), the gestational sac is well-established and clearly visible. - At this point, a **yolk sac** is almost always present within the gestational sac, and often a **fetal pole** may be identified. - This represents a later stage, not the *first* time the gestational sac can be detected. *49 days* - By **49 days** (7 weeks gestational age), not only is the **gestational sac** clearly visible, but a **yolk sac** and **fetal pole** with **cardiac activity** are typically identifiable. - This time frame represents a much later stage of pregnancy visualization, well beyond the initial appearance of the gestational sac.
Question 28: A 30-year-old housewife reports with 6 months amenorrhea. Her serum LH and FSH are high with low estradiol levels. What is the most likely cause of amenorrhea in this context?
- A. Premature menopause (Correct Answer)
- B. Polycystic ovarian disease
- C. Exercise induced
- D. Pituitary tumour
Explanation: ***Premature menopause*** - **High LH and FSH** with **low estradiol** levels indicate primary ovarian failure, where the ovaries are no longer responding to pituitary stimulation. - In a 30-year-old woman, this ovarian failure presenting as 6 months of amenorrhea is consistent with **premature menopause** (also known as premature ovarian insufficiency). *Polycystic ovarian disease* - Characterized by **high LH:FSH ratio** (typically LH higher than FSH) and **high estrogen** due to peripheral conversion of androgens, which is contrary to the low estradiol observed here. - Presents with features like **hirsutism**, acne, and menstrual irregularities, but typically not with primary ovarian failure. *Exercise induced* - **Exercise-induced amenorrhea** (hypothalamic amenorrhea) is characterized by **low or normal LH and FSH** and **low estradiol**, reflecting inadequate GnRH pulsatility from the hypothalamus, not primary ovarian failure. - This condition is a form of **secondary amenorrhea** due to a disruption in the hypothalamic-pituitary-ovarian axis, often seen in athletes or people with low body fat. *Pituitary tumour* - A **pituitary tumor** can cause amenorrhea by various mechanisms, such as secreting prolactin (prolactinoma) which **inhibits GnRH**, leading to **low LH, FSH, and estradiol**. - Alternatively, a large non-functional tumor might cause hypopituitarism, also resulting in **low gonadotropins and estradiol**, which contradicts the high LH and FSH seen in this patient.
Question 29: The Pearl index of contraceptive failure is expressed as a rate per
- A. 1000 women-years
- B. 1 woman-year
- C. 10 women-years
- D. 100 women-years (Correct Answer)
Explanation: ***100 women-years*** - The **Pearl Index** is a common measure of contraceptive failure rate, expressed as the number of pregnancies per **100 women-years** of exposure. - This metric allows for standardized comparison of contraceptive effectiveness across different methods and populations. *1000 women-years* - While other epidemiological rates might be expressed per 1000 person-years, the standard for the **Pearl Index** is specifically per 100 women-years. - Using 1000 would significantly underestimate the commonly reported failure rates of contraceptives. *1 woman-year* - Expressing the rate per **1 woman-year** would result in very small, often fractional, numbers that are difficult to interpret and compare. - The larger base of 100 women-years provides a more practical and understandable scale for reporting contraceptive failure. *10 women-years* - This increment is not the recognized standard for the **Pearl Index**. - Using 10 women-years would also make the reported failure rates less comparable with established data and harder to interpret clinically.
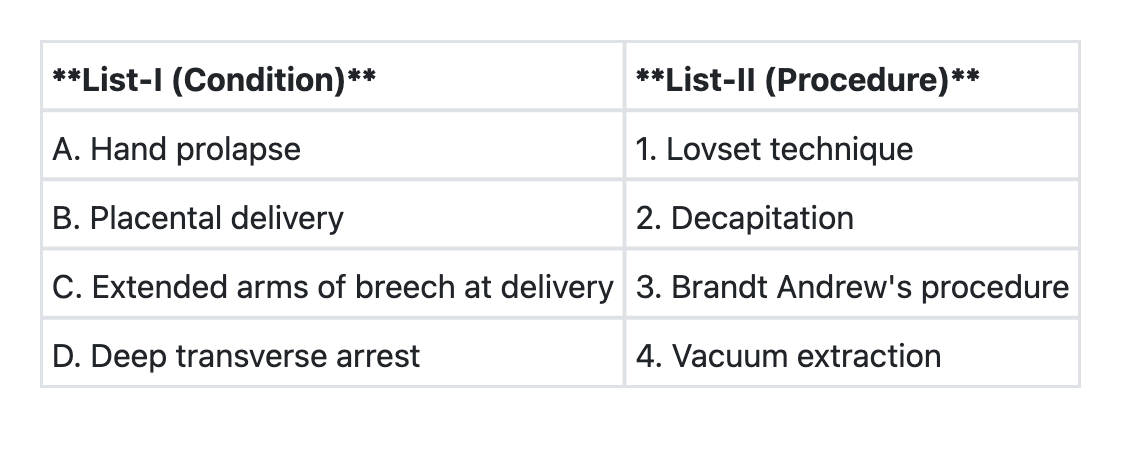
Question 30: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→4 B→1 C→3 D→2
- B. A→2 B→1 C→3 D→4
- C. A→2 B→3 C→1 D→4 (Correct Answer)
- D. A→4 B→3 C→1 D→2
Explanation: ***A→2 B→3 C→1 D→4*** - **Hand prolapse (A)** occurs when a fetal hand prolapses alongside the presenting part, leading to obstructed labor. If the fetus is dead and vaginal delivery is impossible due to severe obstruction, **Decapitation (2)** may be performed as a destructive procedure to facilitate delivery. - **Placental delivery (B)** is managed by the **Brandt-Andrews maneuver (3)**, which involves controlled cord traction with counter-pressure on the uterus to prevent uterine inversion and facilitate safe placental separation. - **Extended arms of breech at delivery (C)** occurs when the fetal arms are extended above the head during breech presentation. The **Lovset maneuver (1)** is specifically designed to deliver extended arms by rotating the fetus to bring the posterior arm down and anteriorly. - **Deep transverse arrest (D)** occurs when the fetal head arrests in the transverse diameter of the pelvis. **Forceps delivery or vacuum extraction (4)** can be used with manual or instrumental rotation to deliver the fetal head. *A→4 B→1 C→3 D→2* - This incorrectly matches hand prolapse with vacuum extraction, which cannot address the obstruction caused by a prolapsed hand. It also reverses the Brandt-Andrews maneuver and Lovset technique. *A→2 B→1 C→3 D→4* - This incorrectly matches placental delivery with Lovset technique (which is for breech) and extended arms with Brandt-Andrews maneuver (which is for placental delivery). *A→4 B→3 C→1 D→2* - This incorrectly matches hand prolapse with vacuum extraction and deep transverse arrest with decapitation. Decapitation is not indicated for deep transverse arrest, which can be managed with forceps or vacuum.