UPSC-CMS 2014 — Obstetrics and Gynecology
30 Previous Year Questions with Answers & Explanations
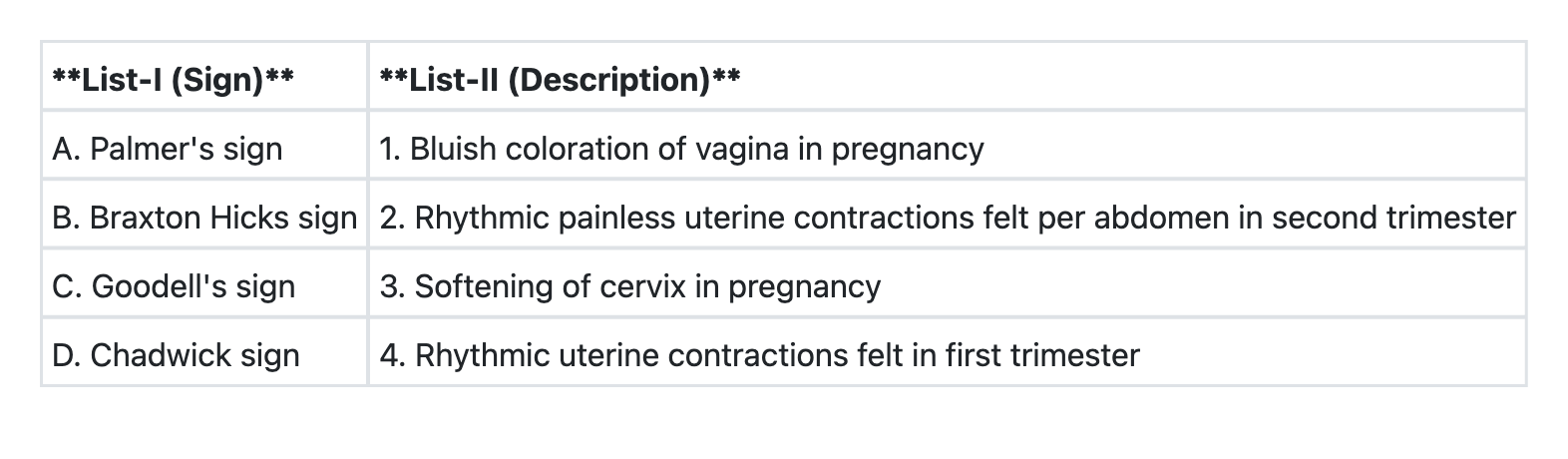
Match List-I with List-II and select the correct answer using the code given below the Lists:
HELLP syndrome includes the following except:
Predisposing factors of puerperal sepsis are following except:
Consider the following: 1. Fetal pulmonary hypoplasia 2. Fetal chromosomal anomalies 3. Prostaglandin synthetase inhibitors 4. Amniotic fluid index of 15 cm Which of the above are associated with oligohydramnios?
Surgical treatment of choice for a 20 year old nulliparous woman with uterine prolapse is:
A 32 years old woman with two live children was brought to emergency with history of missed period for 15 days, spotting since 7 days and pain abdomen since 6 hours. Her pulse was 120 per minute, pallor + +, systolic B.P. 80 mm Hg. There was fullness and tenderness on per abdomen examination. Copper T thread was seen through external os on per speculum examination. On p/ v examination, cervical movements were tender, uterus was anteverted, bulky and soft. There was fullness in pouch of Douglas. Most likely, she is suffering from:
A 20 year old primigravida is admitted with full term pregnancy and labour pains. At 4 A.M. she goes into active phase of labour with 4 cm cervical dilatation. Membranes rupture during p/v examination showing clear liquor. A repeat p/v after 4 hours of good uterine contractions reveals a cervical dilatation of 5 cm. What should be the next step in management?
Immediately after third stage of labour in a case of full term delivery, the fundus of the uterus is:
Which one of the following is not a complication of shoulder dystocia?
Which of the following methods for induction of labour should not be used in the patient with previous lower segment caesarean section?
UPSC-CMS 2014 - Obstetrics and Gynecology UPSC-CMS Practice Questions and MCQs
Question 1: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→1 B→2 C→3 D→4
- B. A→4 B→2 C→3 D→1 (Correct Answer)
- C. A→3 B→2 C→1 D→4
- D. A→2 B→3 C→1 D→4
Explanation: ***A→4 B→2 C→3 D→1*** - **Palmer's sign** refers to **rhythmic uterine contractions** felt by bimanual examination in the **first trimester** of pregnancy. This is often an early sign used to detect pregnancy. - **Braxton Hicks contractions** are characterized by **rhythmic, painless uterine contractions** that are felt per abdomen and typically occur in the **second and third trimesters** of pregnancy. They are often called "practice contractions." - **Goodell's sign** describes the **softening of the cervix** in early pregnancy due to increased vascularity and edema. - **Chadwick's sign** is the **bluish coloration of the vagina and cervix** in pregnancy, also due to increased vascularity and blood flow. *A→1 B→2 C→3 D→4* - This option incorrectly matches Palmer's sign with bluish coloration of the vagina, which is **Chadwick's sign**. - It also incorrectly matches Chadwick's sign with rhythmic uterine contractions in the first trimester, which is **Palmer's sign**. *A→3 B→2 C→1 D→4* - This option incorrectly matches Palmer's sign with softening of the cervix (**Goodell's sign**) and Goodell's sign with bluish coloration of the vagina (**Chadwick's sign**). - It also incorrectly matches Chadwick's sign with rhythmic uterine contractions in the first trimester (**Palmer's sign**). *A→2 B→3 C→1 D→4* - This option incorrectly matches Palmer's sign with Braxton Hicks contractions and Braxton Hicks sign with softening of the cervix, which is **Goodell's sign**. - It also incorrectly matches Goodell's sign with bluish coloration of the vagina (**Chadwick's sign**) and Chadwick's sign with rhythmic contractions in the first trimester (**Palmer's sign**).
Question 2: HELLP syndrome includes the following except:
- A. Low platelet count
- B. Leucocytosis (Correct Answer)
- C. Hemolysis
- D. Elevated liver enzymes
Explanation: ***Leucocytosis*** - HELLP syndrome is characterized by **hemolysis**, **elevated liver enzymes**, and **low platelet count**. Leucocytosis (an elevated white blood cell count) is **not a defining feature** of HELLP syndrome. - While leucocytosis can occur in conditions associated with inflammation or stress, it is **not a diagnostic criterion** for HELLP syndrome and doesn't represent one of its core components. *Low platelet count* - **Thrombocytopenia** (platelet count below 100,000/microL) is a critical component of HELLP syndrome, representing the "LP" in the acronym. - It results from increased platelet consumption and destruction due to widespread endothelial dysfunction. *Hemolysis* - **Hemolysis** (breakdown of red blood cells) is the "H" in the HELLP acronym. - It is evidenced by findings such as **schistocytes** on peripheral blood smear, elevated **lactate dehydrogenase (LDH)**, and unconjugated **hyperbilirubinemia**. *Elevated liver enzymes* - **Elevated liver enzymes** (e.g., aspartate aminotransferase (AST) and alanine aminotransferase (ALT) being at least twice the upper limit of normal) are the "EL" in HELLP. - This elevation indicates **hepatic dysfunction** and hepatocellular damage, often associated with periportal hemorrhage and fibrin deposition.
Question 3: Predisposing factors of puerperal sepsis are following except:
- A. Multiparity (Correct Answer)
- B. Placenta previa
- C. Cases of manual removal of placenta
- D. Repeated internal examinations specially in the case of premature rupture of membrane
Explanation: ***Multiparity*** - **Multiparity**, defined as having given birth to more than one child, is generally considered a protective factor rather than a predisposing factor for puerperal sepsis. - While it was historically associated with some obstetric complications, modern evidence does not support it as a direct risk factor for puerperal sepsis. *Placenta previa* - **Placenta previa** increases the risk of hemorrhage and the need for interventions such as manual removal of the placenta or cesarean section, all of which elevate the risk of infection. - The abnormal placental implantation itself can lead to a more traumatic delivery and exposure to infection. *Cases of manual removal of placenta* - **Manual removal of the placenta** involves direct digital exploration of the uterine cavity, which introduces bacteria into a potentially sterile environment. - This procedure also causes trauma to the uterine lining, creating an entry point for infection. *Repeated internal examinations specially in the case of premature rupture of membrane* - **Repeated internal examinations**, especially after **premature rupture of membranes (PROM)**, repeatedly introduce microorganisms from the vagina into the sterile uterine cavity. - PROM itself removes the protective barrier against ascending infection, making frequent examinations particularly risky.
Question 4: Consider the following: 1. Fetal pulmonary hypoplasia 2. Fetal chromosomal anomalies 3. Prostaglandin synthetase inhibitors 4. Amniotic fluid index of 15 cm Which of the above are associated with oligohydramnios?
- A. 2, 3 and 4
- B. 1, 2 and 4
- C. 1, 2 and 3 (Correct Answer)
- D. 1, 3 and 4
Explanation: ***1, 2 and 3*** - **Fetal pulmonary hypoplasia** is associated with oligohydramnios as a significant **complication** of severe and prolonged oligohydramnios. Reduced amniotic fluid impairs normal fetal breathing movements and lung expansion, leading to pulmonary hypoplasia. This is a consequence rather than a cause, but represents an important clinical association. - **Fetal chromosomal anomalies** (such as Turner syndrome, Trisomy 18) can lead to structural renal abnormalities including renal agenesis, multicystic dysplastic kidney, or obstructive uropathy. These conditions result in decreased or absent fetal urine production, which is the primary source of amniotic fluid in the second half of pregnancy, thereby **causing oligohydramnios**. - **Prostaglandin synthetase inhibitors** (e.g., indomethacin, other NSAIDs) decrease fetal renal blood flow and glomerular filtration rate, leading to reduced fetal urine output. This effect is particularly significant when used in the third trimester, and can **cause oligohydramnios**. *2, 3 and 4* - While fetal chromosomal anomalies and prostaglandin synthetase inhibitors are correctly associated with oligohydramnios as causative factors, **Amniotic fluid index (AFI) of 15 cm** represents a **normal value**. Normal AFI ranges from 8-18 cm (or 5-25 cm by some references), and oligohydramnios is defined as AFI <5 cm. Therefore, AFI of 15 cm is not associated with oligohydramnios. - This option is incorrect because it excludes fetal pulmonary hypoplasia, which has a well-established association with oligohydramnios. *1, 2 and 4* - This option incorrectly includes **AFI of 15 cm**, which is within normal range and not associated with oligohydramnios. - While fetal pulmonary hypoplasia and fetal chromosomal anomalies are correctly associated with oligohydramnios, the inclusion of a normal AFI value makes this option incorrect. *1, 3 and 4* - This option incorrectly includes **AFI of 15 cm**, which is a normal finding that indicates adequate amniotic fluid volume, not oligohydramnios. - Although fetal pulmonary hypoplasia and prostaglandin synthetase inhibitors are associated with oligohydramnios, the inclusion of normal AFI makes this option incorrect.
Question 5: Surgical treatment of choice for a 20 year old nulliparous woman with uterine prolapse is:
- A. Sacrocolpopexy (Correct Answer)
- B. Le Forte’s repair
- C. Sling surgery
- D. Abdominal hysterectomy with pelvic floor repair
Explanation: ***Sacrocolpopexy (Sacrohysteropexy variant)*** - For a **young, nulliparous woman**, the procedure of choice is **sacrohysteropexy** (also called sacrocervicopexy), which involves attaching the **uterus/cervix** to the **sacrum** using synthetic mesh, providing durable support while preserving the uterus. - This is ideal for young women as it **preserves fertility potential** and maintains vaginal length and sexual function. - The term sacrocolpopexy in this context refers to the uterine-preserving variant, crucial for women desiring future pregnancy. *Le Forte's repair* - This is an **obliterative procedure** primarily used in elderly women who are **no longer sexually active**, involving partial closure of the vagina. - It is absolutely contraindicated in a young, nulliparous woman who desires future sexual function and pregnancy. *Sling surgery* - **Sling surgery** is primarily indicated for **stress urinary incontinence**, not uterine prolapse. - While incontinence can co-exist with prolapse, a sling alone does not address uterine or vaginal apex support. *Abdominal hysterectomy with pelvic floor repair* - **Hysterectomy** removes the uterus and would **eliminate fertility**, which is unacceptable for a young, nulliparous woman desiring children. - Though effective for prolapse, it is an overly aggressive approach; uterine-preserving procedures like sacrohysteropexy are strongly preferred for fertility preservation.
Question 6: A 32 years old woman with two live children was brought to emergency with history of missed period for 15 days, spotting since 7 days and pain abdomen since 6 hours. Her pulse was 120 per minute, pallor + +, systolic B.P. 80 mm Hg. There was fullness and tenderness on per abdomen examination. Copper T thread was seen through external os on per speculum examination. On p/ v examination, cervical movements were tender, uterus was anteverted, bulky and soft. There was fullness in pouch of Douglas. Most likely, she is suffering from:
- A. Pelvic inflammatory disease
- B. Ruptured ectopic pregnancy (Correct Answer)
- C. Missed abortion with infection
- D. Threatened abortion
Explanation: ***Ruptured ectopic pregnancy*** - The patient presents with **classic signs of ruptured ectopic pregnancy**: missed period, vaginal spotting, acute abdominal pain, **hypovolemic shock** (tachycardia, hypotension, pallor), and signs of internal bleeding (abdominal fullness, tenderness, cervical motion tenderness, fullness in the pouch of Douglas). - The presence of a **Copper T IUD** further increases the risk of ectopic pregnancy if conception occurs, as IUDs are highly effective at preventing intrauterine pregnancies but less so at preventing ectopic ones. *Pelvic inflammatory disease* - While PID can cause abdominal pain and cervical motion tenderness, it is usually associated with **fever, purulent vaginal discharge**, and a history of sexually transmitted infections, which are not mentioned here. - The **acute hemodynamic instability** (shock) and history of missed period are not typical features of uncomplicated PID. *Missed abortion with infection* - A missed abortion involves a non-viable pregnancy with a closed cervix, and while infection can occur, it typically presents with **fever, foul-smelling discharge**, and abdominal pain that is less acute and severe than seen in this case. - The profound shock and localized fullness in the pouch of Douglas are more indicative of **hemoperitoneum** from a ruptured ectopic pregnancy rather than an infected missed abortion. *Threatened abortion* - Threatened abortion is characterized by vaginal bleeding with a **closed cervix** and a **viable intrauterine pregnancy**, usually without severe pain or signs of shock. - The patient's **hemodynamic instability**, severe abdominal pain, and findings suggestive of internal bleeding rule out a simple threatened abortion.
Question 7: A 20 year old primigravida is admitted with full term pregnancy and labour pains. At 4 A.M. she goes into active phase of labour with 4 cm cervical dilatation. Membranes rupture during p/v examination showing clear liquor. A repeat p/v after 4 hours of good uterine contractions reveals a cervical dilatation of 5 cm. What should be the next step in management?
- A. Oxytocin drip
- B. Reassess for occipitoposterior position and cephalopelvic disproportion (Correct Answer)
- C. Immediate caesarean section
- D. Reassess after 4 hours
Explanation: ***Reassess for occipitoposterior position and cephalopelvic disproportion*** - The patient has **protracted active phase** with only 1 cm cervical dilatation in 4 hours (from 4 cm to 5 cm), which is significantly slower than the expected rate of at least 1 cm/hour in primigravidas. - Crucially, the question states she has **"good uterine contractions"**, which means the slow progress is NOT due to inadequate uterine activity. - When labor progress is slow DESPITE adequate contractions, this indicates a **mechanical obstruction** such as occipitoposterior position, cephalopelvic disproportion, asynclitism, or other malpresentation. - The next step is to **assess for these mechanical factors** through clinical examination (abdominal palpation, vaginal examination to assess position, station, molding, caput) before considering augmentation. - **Augmentation with oxytocin is contraindicated** when contractions are already adequate, as it may lead to uterine hyperstimulation without improving progress if there's mechanical obstruction. *Oxytocin drip* - Oxytocin augmentation is indicated for **hypotonic uterine dysfunction** (inadequate contractions causing slow progress). - In this case, contractions are described as **"good"**, so oxytocin is NOT appropriate as the first-line intervention. - Using oxytocin when contractions are already adequate without first ruling out mechanical obstruction can be dangerous and may lead to uterine rupture or fetal compromise. *Immediate caesarean section* - While caesarean section may ultimately be needed if mechanical obstruction is confirmed, it is **premature** without first assessing the cause of slow progress. - A diagnosis must be established before proceeding to operative delivery. *Reassess after 4 hours* - Further expectant management without intervention or diagnosis is **inappropriate** as the patient has already demonstrated inadequate progress. - Prolonged labor increases risks of maternal exhaustion, infection, and fetal compromise. - Active management requires diagnosis and intervention, not continued observation.
Question 8: Immediately after third stage of labour in a case of full term delivery, the fundus of the uterus is:
- A. At the level of xiphisternum
- B. Below the level of umbilicus
- C. At the level of umbilicus (Correct Answer)
- D. Just above the symphysis pubis
Explanation: ***At the level of umbilicus*** - Immediately after delivery of the placenta (third stage of labor), the **fundus** typically contracts down to the level of the **umbilicus**. - This contraction helps to compress uterine blood vessels and prevent **postpartum hemorrhage**. *At the level of xiphisternum* - The uterus reaches the **xiphisternum** only in late third trimester, as the fetus grows. - After delivery, the uterus significantly reduces in size, so it would not remain this high. *Below the level of umbilicus* - While the uterus will eventually descend below the umbilicus during **involution** (shrinking back to pre-pregnancy size), this process takes several days to weeks, not immediately after delivery. - A fundus below the umbilicus immediately after delivery might suggest a failure of proper contraction. *Just above the symphysis pubis* - The uterus is at the level of the **symphysis pubis** much earlier in pregnancy, typically around **12 weeks gestation**. - A fundus at this level immediately after delivery would indicate an abnormally small uterus or an incomplete emptying.
Question 9: Which one of the following is not a complication of shoulder dystocia?
- A. Brachial plexus palsy
- B. Placental abruption (Correct Answer)
- C. Postpartum haemorrhage
- D. Facial palsy
Explanation: ***Placental abruption*** - **Placental abruption** is the premature detachment of the placenta from the uterine wall, typically occurring before or during labour. It is not directly caused by the mechanical obstruction during shoulder dystocia. - Complications of shoulder dystocia are primarily related to mechanical forces exerted on the baby and mother during delivery, such as nerve injuries or uterine atony, not placental conditions. *Brachial plexus palsy* - **Brachial plexus palsy** is a common complication of shoulder dystocia, often resulting from excessive lateral traction on the fetal head or neck during delivery. - This traction can stretch or tear the nerves of the brachial plexus, leading to varying degrees of paralysis or weakness in the arm and hand. *Postpartum haemorrhage* - **Postpartum haemorrhage** is a significant risk following shoulder dystocia due to the prolonged and often traumatic nature of the delivery. - The increased manipulation and potential for uterine atony or soft tissue trauma during resolution of shoulder dystocia can predispose the mother to excessive bleeding. *Facial palsy* - **Facial palsy** can occur during shoulder dystocia if there is compression or stretching of the facial nerve (cranial nerve VII) against the maternal pelvis or other structures during delivery. - While less common than brachial plexus palsy, it can result from the abnormal forces and positions during a difficult shoulder dystocia delivery.
Question 10: Which of the following methods for induction of labour should not be used in the patient with previous lower segment caesarean section?
- A. Stripping of the membrane
- B. Oxytocin drip
- C. Vaginal prostaglandin gel (Correct Answer)
- D. Oral prostaglandin tablet
Explanation: ***Vaginal prostaglandin gel*** - **Prostaglandins** (especially **PGE2 vaginal gel**) are **absolutely contraindicated** for induction of labor in women with a previous lower segment caesarean section (LSCS). - They cause strong, sustained uterine contractions that significantly increase the risk of **uterine rupture** in a scarred uterus. - This is the **most established and widely recognized contraindication** among induction methods for VBAC candidates. - **PGE2 vaginal preparations** have the highest documented risk of uterine rupture (1-2% or higher) in scarred uteri. *Stripping of the membrane* - This method involves separating the **chorioamniotic membranes** from the lower uterine segment, which can release natural prostaglandins. - It is generally considered **safe** in women with a previous LSCS as it causes only mild, physiologic uterine activity. - Does not directly stimulate strong, unphysiologic uterine contractions like exogenous prostaglandins. *Oxytocin drip* - **Oxytocin** can be used cautiously for induction of labor in women with a previous LSCS, with close fetal and contraction monitoring. - While it can cause strong contractions, its effect is **titratable** and can be stopped immediately if hyperstimulation occurs. - It is the **preferred pharmacological method** for induction in trial of labor after cesarean (TOLAC). - Careful dose titration and continuous monitoring make it safer than prostaglandins for this indication. *Oral prostaglandin tablet* - **Oral misoprostol** also carries significant risk of uterine hyperstimulation in patients with a scarred uterus and is generally avoided in previous LSCS. - However, vaginal prostaglandin preparations are considered the **primary contraindication** in most guidelines and examination contexts due to more extensive documentation of rupture risk and less controllable absorption. - While both prostaglandin routes are problematic, vaginal gel represents the most established contraindication for VBAC induction.