UPSC-CMS 2014 — Internal Medicine
10 Previous Year Questions with Answers & Explanations
Which is the most commonly used chemotherapy regimen in the adjuvant treatment following modified radical mastectomy in the estrogen receptor negative 35 year old female with breast cancer?
Consider the following statements: The clinical features of tension pneumothorax include 1. tracheal shift to contralateral side 2. absent breath sounds on the affected side 3. low output circulatory failure 4. peripheral cyanosis Which of the statements given above is/are correct?
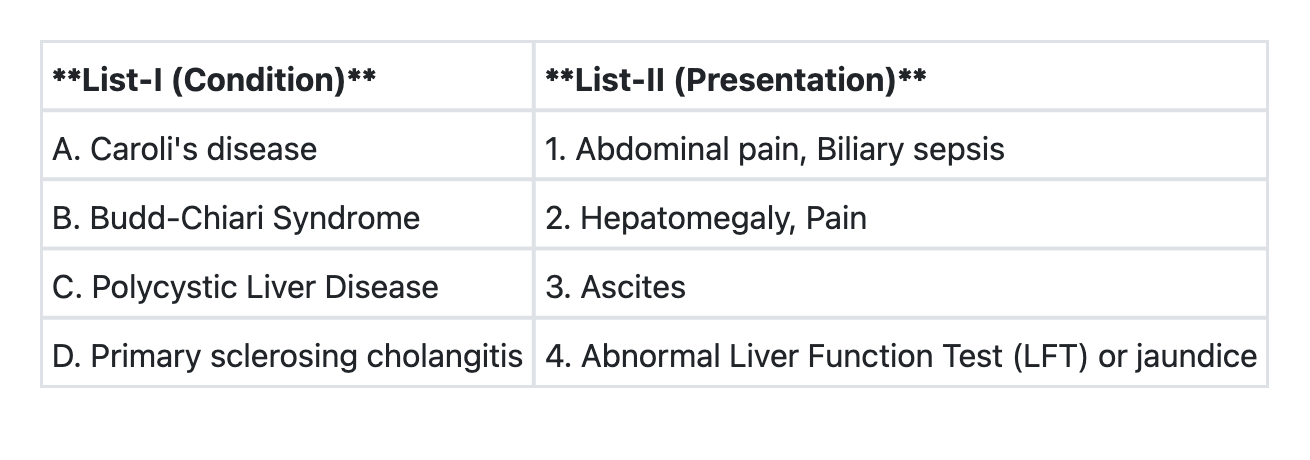
Match List-I with List-II and select the correct answer using the code given below the Lists:
The following are features of hypovolemic shock except:
A 45 year old man sustains trauma in a road traffic accident and develops engorgement of neck veins, pallor, rapid pulse rate, and chest pain. What is the most likely diagnosis?
Which one of the following statements is not correct regarding trichobezoar ( hair balls)?
Which one of the following is given a score of two in Alvarado score?
Tuberculosis in HIV positive individuals is characterized by which of the following? 1. More frequent negative sputum smears. 2. More false–negative tuberculin test results. 3. More extra–pulmonary tuberculosis. 4. More cavitating lesions in lungs as shown by chest X-ray. Select the correct answer using the code given below:
Consider the following features of cholera: 1. Onset with purging. 2. No nausea or retching. 3. No tenesmus. 4. Leukocytosis. Which of the above features of cholera differentiate it from food poisoning?
Which of the following statements is not true regarding HIV infection?
UPSC-CMS 2014 - Internal Medicine UPSC-CMS Practice Questions and MCQs
Question 1: Which is the most commonly used chemotherapy regimen in the adjuvant treatment following modified radical mastectomy in the estrogen receptor negative 35 year old female with breast cancer?
- A. Adriamycin + 5-Fluorouracil
- B. Cyclophosphamide + Adriamycin + 5-Fluorouracil (Correct Answer)
- C. Cyclophosphamide + 5-Fluorouracil
- D. Cyclophosphamide + Methotrexate + 5-Fluorouracil
Explanation: ***Cyclophosphamide + Adriamycin + 5-Fluorouracil*** - The **CAF** (Cyclophosphamide, Adriamycin, 5-Fluorouracil) or **FAC** regimen is a widely used and effective **combination chemotherapy** for adjuvant treatment in **ER-negative breast cancer**, offering a robust approach to systemic control. - This regimen addresses the aggressive nature of **ER-negative tumors**, for which **endocrine therapy** is not an option, and aims to eradicate micrometastases reducing recurrence risk. *Adriamycin + 5-Fluorouracil* - While both **Adriamycin** and **5-Fluorouracil** are active agents in breast cancer, this two-drug combination in isolation is generally considered less potent than multi-agent regimens, particularly for **ER-negative disease**. - It lacks the additional mechanism of action and efficacy provided by **cyclophosphamide**, which is a key component in many standard regimens for this aggressive tumor subtype. *Cyclophosphamide + 5-Fluorouracil* - This two-drug regimen is not a standard frontline or the most common adjuvant chemotherapy for ER-negative breast cancer due to its relatively lower efficacy compared to regimens that include an **anthracycline** like Adriamycin. - The absence of an **anthracycline** like Adriamycin, which is a powerful agent against breast cancer, limits its overall effectiveness in a setting where aggressive systemic treatment is crucial. *Cyclophosphamide + Methotrexate + 5-Fluorouracil* - The **CMF** (Cyclophosphamide, Methotrexate, 5-Fluorouracil) regimen was historically a foundational adjuvant therapy; however, for **ER-negative breast cancer**, regimens containing an **anthracycline** like Adriamycin are generally preferred due to their superior efficacy. - While effective, **CMF** is often considered less potent than anthracycline-containing regimens like **CAF/FAC** in treating aggressive, **ER-negative tumors**, which typically benefit from the broader cytotoxic activity of an anthracycline.
Question 2: Consider the following statements: The clinical features of tension pneumothorax include 1. tracheal shift to contralateral side 2. absent breath sounds on the affected side 3. low output circulatory failure 4. peripheral cyanosis Which of the statements given above is/are correct?
- A. 1 and 3 only
- B. 1, 2 and 3 (Correct Answer)
- C. 2 and 4
- D. 1 and 4
Explanation: ***1, 2 and 3*** - **Tracheal deviation to the contralateral side** is a hallmark sign of tension pneumothorax [1], caused by the increasing pressure in the affected hemithorax pushing mediastinal structures away. - **Absent breath sounds on the affected side** result from the complete collapse of the lung and inability of air to enter the pleural space with inspiration [1]. **Low output circulatory failure** occurs due to increased intrathoracic pressure compressing the heart and great vessels, impairing venous return and cardiac output [2]. *1 and 3 only* - While **tracheal shift to the contralateral side** and **low output circulatory failure** [2] are indeed features, this option incorrectly excludes **absent breath sounds on the affected side**, which is a critical clinical finding in tension pneumothorax. - The absence of breath sounds directly reflects the collapsed lung, a primary mechanical consequence of the condition. *2 and 4* - **Absent breath sounds on the affected side** is correct, but **peripheral cyanosis** is not a *primary* or *early* distinguishing feature of tension pneumothorax. While hypoxemia can lead to cyanosis, it's often a late and less specific sign. - This option misses the crucial finding of **tracheal deviation** and the systemic impact of **circulatory failure** [2], which are more direct indicators of the severity and mechanism of tension pneumothorax. *1 and 4* - **Tracheal shift to the contralateral side** is a correct feature. However, **peripheral cyanosis** is a less specific and often later sign compared to the direct mechanical and circulatory effects. - This option incorrectly omits **absent breath sounds on the affected side** and **low output circulatory failure**, both of which are more consistently present and diagnostically important in tension pneumothorax.
Question 3: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→1 B→3 C→2 D→4 (Correct Answer)
- B. A→1 B→2 C→3 D→4
- C. A→3 B→2 C→4 D→1
- D. A→4 B→3 C→2 D→1
Explanation: ***A→1 B→3 C→2 D→4*** - Caroli's disease is characterized by **dilatation of intrahepatic bile ducts**, predisposing to **bile stasis**, stone formation, and recurrent **biliary sepsis** with associated abdominal pain. - Budd-Chiari Syndrome is defined by **hepatic venous outflow obstruction**, leading to symptoms like **ascites**, hepatomegaly, and abdominal pain. - Polycystic Liver Disease involves the presence of **multiple cysts in the liver**, which can cause **hepatomegaly** and **pain** due to the size and mass effect of the cysts. - Primary sclerosing cholangitis (PSC) is a **cholestatic liver disease** causing inflammation and fibrosis of the bile ducts, leading to **abnormal liver function tests** (elevated alkaline phosphatase and bilirubin) and often presenting with **jaundice**. *A→1 B→2 C→3 D→4* - This option incorrectly matches Budd-Chiari Syndrome with Hepatomegaly, Pain and Polycystic Liver Disease with Ascites. - The hallmark of Budd-Chiari is venous outflow obstruction leading to **ascites**, while **hepatomegaly and pain** are more characteristic symptoms of Polycystic Liver Disease due to the expanding cysts. *A→3 B→2 C→4 D→1* - This option incorrectly associates Caroli's disease with ascites and Primary Sclerosing Cholangitis with Abdominal pain, Biliary sepsis. - Caroli's disease is primarily characterized by **biliary complications** like cholangitis, not ascites, and ascites is a key feature of Budd-Chiari, not Polycystic Liver Disease. *A→4 B→3 C→2 D→1* - This option incorrectly links Caroli's disease with Abnormal LFT/jaundice generally and Primary Sclerosing Cholangitis with Abdominal pain, Biliary sepsis. - While Caroli's can cause abnormal LFTs and jaundice secondarily to cholangitis, its primary specific presentation involves **recurrent infection (biliary sepsis)**. Primary Sclerosing Cholangitis directly causes **abnormal LFTs and jaundice** due to cholestasis, but it is not commonly associated with abdominal pain and biliary sepsis.
Question 4: The following are features of hypovolemic shock except:
- A. Acidosis
- B. Oliguria
- C. Low Blood Pressure
- D. Bradycardia (Correct Answer)
Explanation: ***Bradycardia*** - Hypovolemic shock typically causes **tachycardia** (increased heart rate) as a compensatory mechanism to maintain cardiac output in the face of reduced blood volume [1]. - **Bradycardia** is generally not a feature of hypovolemic shock unless there are confounding factors or severe terminal stages. *Acidosis* - **Lactic acidosis** is a common feature of hypovolemic shock due to tissue hypoperfusion causing anaerobic metabolism [2]. - Reduced blood flow leads to inadequate oxygen delivery, forcing cells to produce lactic acid. *Oliguria* - **Oliguria** (decreased urine output) occurs in hypovolemic shock as the kidneys attempt to conserve fluid due to reduced renal perfusion. - The body prioritizes blood flow to vital organs, leading to decreased kidney function and urine production. *Low Blood Pressure* - **Hypotension** (low blood pressure) is a hallmark of shock, including hypovolemic shock, resulting from a significant reduction in circulating blood volume [1]. - The decrease in blood volume directly reduces venous return, stroke volume, and ultimately, systemic blood pressure.
Question 5: A 45 year old man sustains trauma in a road traffic accident and develops engorgement of neck veins, pallor, rapid pulse rate, and chest pain. What is the most likely diagnosis?
- A. Cardiac tamponade (Correct Answer)
- B. Haemothorax
- C. Pulmonary laceration
- D. Rupture of spleen
Explanation: ***Cardiac tamponade*** - The classic triad of **Beck's triad** (engorged neck veins, muffled heart sounds, and hypotension) along with **tachycardia** and **pallor** in a trauma setting is highly indicative of cardiac tamponade [1]. - **Chest pain** due to pressure on the heart and surrounding structures further supports this diagnosis. *Haemothorax* - While blunt trauma can cause **haemothorax**, it typically presents with **diminished or absent breath sounds** on the affected side and **respiratory distress**, not prominently with engorged neck veins unless it's very large and significantly compromises venous return. - The primary sign would be **hypotension** and **tachycardia** from hypovolemia, but without the JVD. *Pulmonary laceration* - A pulmonary laceration would primarily cause **pneumothorax** or **haemothorax**, leading to signs like **dyspnea**, **chest pain**, and potentially **subcutaneous emphysema**. - **Engorged neck veins** are not a primary feature unless the resulting pneumothorax is tension type, which would also present with tracheal deviation. *Rupture of spleen* - A ruptured spleen causes **internal bleeding** (hypovolemic shock) presenting as **abdominal pain**, **left upper quadrant tenderness**, **tachycardia**, and **hypotension**. - **Engorged neck veins** are not a characteristic symptom of splenic rupture because it is a source of blood loss leading to hypovolemia.
Question 6: Which one of the following statements is not correct regarding trichobezoar ( hair balls)?
- A. It is associated usually with psychiatric illness.
- B. It is usually associated with pyloric stenosis. (Correct Answer)
- C. It is more common in females.
- D. It is more common in young.
Explanation: ***It is usually associated with pyloric stenosis.*** - **Trichobezoars** are generally not associated with **pyloric stenosis**. The two conditions have distinct etiologies and pathophysiologies. - While both can present with gastric outlet obstruction symptoms, the presence of a hairball does not imply an underlying congenital or acquired narrowing of the pylorus. *It is associated usually with psychiatric illness.* - **Trichobezoars** are highly associated with **trichophagia** (compulsive hair eating), which is often a symptom of underlying psychiatric conditions like **trichotillomania** or **pica**. - These conditions involve an irresistible urge to pull out one's hair and/or consume non-nutritive substances, including hair. *It is more common in females.* - **Trichobezoars** are indeed more commonly found in **females**, especially young females [1]. - This increased prevalence is often linked to the higher incidence of **trichotillomania** and **trichophagia** in females. *It is more common in young.* - **Trichobezoars** are observed more frequently in **children and adolescents**, particularly among young girls [1]. - The behaviors of **trichotillomania** and **trichophagia** often develop during childhood or early adolescence [1].
Question 7: Which one of the following is given a score of two in Alvarado score?
- A. Leukocytosis (Correct Answer)
- B. Anorexia
- C. Pyrexia
- D. Rebound tenderness
Explanation: ***Leukocytosis*** - A **leukocyte count greater than 10,000/mm³** (leukocytosis) is assigned a score of **two points** in the Alvarado score. [2] - This parameter reflects the systemic inflammatory response often associated with acute appendicitis. [1] *Anorexia* - **Anorexia**, or loss of appetite, is a common symptom in acute appendicitis but is only assigned **one point** in the Alvarado score. - It is a non-specific symptom that can be present in numerous conditions. *Pyrexia* - **Pyrexia** (fever) is another indicator of inflammation, but in the Alvarado score, a **fever of 37.3°C or higher** is given only **one point**. - This symptom, while important, does not carry the same weight as a significant elevation in white blood cell count. *Rebound tenderness* - **Rebound tenderness** is a sign of peritoneal irritation and is given **one point** in the Alvarado score. [1] - While strongly correlated with appendicitis, it is a clinical finding rather than a laboratory marker.
Question 8: Tuberculosis in HIV positive individuals is characterized by which of the following? 1. More frequent negative sputum smears. 2. More false–negative tuberculin test results. 3. More extra–pulmonary tuberculosis. 4. More cavitating lesions in lungs as shown by chest X-ray. Select the correct answer using the code given below:
- A. 1, 2, 3 and 4
- B. 1 and 2 only
- C. 3 and 4 only
- D. 1, 2 and 3 only (Correct Answer)
Explanation: ***1, 2, and 3 only*** - HIV coinfection impairs cell-mediated immunity, leading to **atypical presentations** of TB [1]. All three options (more frequent negative sputum smears, more false-negative tuberculin tests, and more extrapulmonary TB) are characteristic of TB in HIV-positive individuals due to this **immunodeficiency** [2]. - The immunocompromised state often results in a **diminished inflammatory response**, making diagnosis more challenging and dissemination more likely. *1, 2, 3 and 4* - This option incorrectly includes "more cavitating lesions in lungs as shown by chest X-ray" as a characteristic feature. HIV-positive individuals, particularly those with advanced immunodeficiency, tend to have **fewer cavitating lesions** because their immune system is less capable of mounting the robust inflammatory response required for cavitation [1]. - Cavitation is more typical of **immunocompetent** individuals with pulmonary TB [1]. *3 and 4 only* - This option is incorrect because, while **more extrapulmonary tuberculosis** is characteristic, **more cavitating lesions** are generally not observed in HIV-positive individuals; in fact, the opposite is true. - The combination of these two points together makes this option largely inaccurate. *1 and 2 only* - While **more frequent negative sputum smears** and **false-negative tuberculin tests** [2] are indeed characteristic, this option is incomplete as it misses the increased prevalence of **extrapulmonary TB** [3], which is a significant feature in HIV-positive individuals. - HIV-related immunodeficiency often leads to the widespread dissemination of *Mycobacterium tuberculosis* outside the lungs [3].
Question 9: Consider the following features of cholera: 1. Onset with purging. 2. No nausea or retching. 3. No tenesmus. 4. Leukocytosis. Which of the above features of cholera differentiate it from food poisoning?
- A. 2, 3 and 4
- B. 1, 2 and 3 (Correct Answer)
- C. 1, 2 and 4
- D. 1, 2, 3 and 4
Explanation: ***1, 2 and 3*** - **Cholera** classically presents with abrupt onset of **painless, watery diarrhea** (purging), often described as "rice-water" stools, typically without significant nausea, retching, or tenesmus [1], [2]. Food poisoning caused by bacterial toxins often involves **nausea, vomiting**, and sometimes abdominal cramps and tenesmus, making features 1, 2, and 3 distinguishing [1], [2]. - The absence of significant inflammation in cholera, unlike many forms of food poisoning, also means that systemic inflammatory markers and symptoms like **fever** are less prominent, and there is no **leukocytosis**. *2, 3 and 4* - This option incorrectly includes the absence of **leukocytosis** as a differentiating feature when food poisoning can also be non-inflammatory, and it omits the crucial feature of **onset with purging**, which is highly characteristic of cholera [1]. - While lack of nausea/retching and tenesmus are key, including leukocytosis as a differentiator without considering other factors is misleading. *1, 2 and 4* - This option misses the absence of **tenesmus** (3), which is a key differentiating feature where **cholera** typically causes painless, watery stools without the straining associated with inflammatory bowel conditions or some types of food poisoning [1], [2]. - It also includes **leukocytosis** (4), which is typically absent in cholera but can be present or absent in food poisoning depending on the cause, making it less specific for differentiation than other features. *1, 2, 3 and 4* - While features 1, 2, and 3 are indeed differentiating, feature 4, **leukocytosis**, is **incorrect** as a differentiating factor in the context of cholera. Cholera typically does not cause leukocytosis because it is a non-inflammatory enterotoxin-mediated illness. - Many forms of food poisoning, especially those mediated by toxins or non-invasive bacteria, also do not cause significant leukocytosis.
Question 10: Which of the following statements is not true regarding HIV infection?
- A. All HIV positive mothers transmit infection to their newborn children. (Correct Answer)
- B. Infected blood transfusion leads to 100% transmission among recipients.
- C. Every HIV infected person would require antiretroviral treatment during lifetime.
- D. HIV does not transmit through fomites.
Explanation: ***All HIV positive mothers transmit infection to their newborn children*** - While **vertical transmission** from mother to child is a significant risk, it is not 100% [1]. With proper antenatal care, **antiretroviral therapy (ART)**, and interventions like elective C-sections or avoiding breastfeeding, the transmission rate can be reduced to less than 1% [1]. - This statement is **false** because various preventative measures can significantly lower the risk of transmission. *Infected blood transfusion leads to 100% transmission among recipients* - This statement is **true**. Although rare due to improved screening, if blood containing HIV is transfused, the recipient will almost certainly become infected due to the direct route of entry of a high viral load directly into the bloodstream [1]. - The high viral load and direct intravascular inoculation bypass natural barriers, making transmission virtually guaranteed. *Every HIV infected person would require antiretroviral treatment during lifetime* - This statement is **true**. Current guidelines recommend that all individuals diagnosed with **HIV infection** should start antiretroviral therapy (ART) regardless of CD4 count, to preserve immune function, prevent opportunistic infections, and reduce transmission [2]. - **ART** is a lifelong commitment, as stopping treatment typically leads to viral rebound and disease progression. *HIV does not transmit through fomites* - This statement is **true**. HIV is a fragile virus that cannot survive long outside the human body and is not transmitted via casual contact or inanimate objects (**fomites**) like doorknoobs, toilet seats, or shared utensils. - Transmission primarily occurs through **blood, semen, pre-ejaculate, rectal fluids, vaginal fluids, and breast milk** [1].