Q11
Excessive nitrates in drinking water can produce:
Q12
The following statements are correct for healthful school environment except:
Q13
The following are the indicators for assessing the sensitivity of surveillance of polio except:
Q14
What is the most important test to assess the prevalence of tuberculosis infection in a community?
Q15
In a normal curve, the area between one standard deviation on either side of the mean will include:
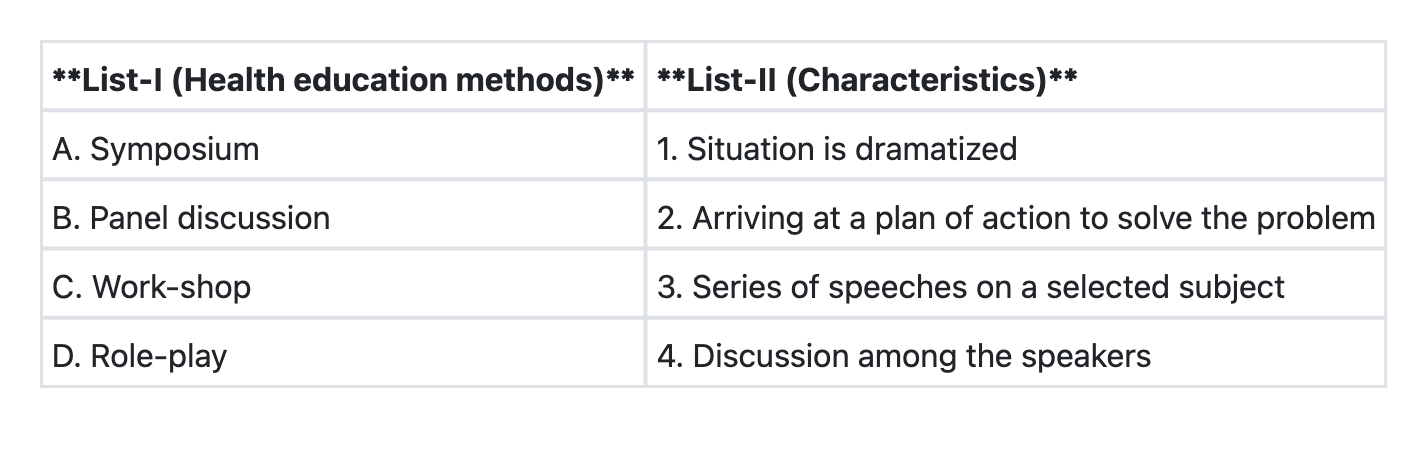
Q16
Match List-I with List-II and select the correct answer using the code given below the Lists:
Q17
Which of the following insecticides is not used as a larvicide?
Q18
An outbreak of Viral Hepatitis was reported from a town between June and August of a particular year. 60% of cases occurred in July. Exposure of the community to infection is from:
Q19
Which one of the following indicators is not included in Millennium Development Goals?
Q20
Severity of a disease is measured by: