UPSC-CMS 2014
113 Previous Year Questions with Answers & Explanations
Dermatology
1 questionsA 40 year old man presented with a flat 1x1cm scaly, itchy black mole on the front of thigh. Examination did not reveal any inguinal lymphodenopathy. The best course of management would be:
UPSC-CMS 2014 - Dermatology UPSC-CMS Practice Questions and MCQs
Question 1: A 40 year old man presented with a flat 1x1cm scaly, itchy black mole on the front of thigh. Examination did not reveal any inguinal lymphodenopathy. The best course of management would be:
- A. FNAC of lesion
- B. Incision biopsy
- C. Wide excision with inguinal lymphadenectomy
- D. Excision biopsy (Correct Answer)
Explanation: ***Excision biopsy*** - A **flat, scaly, itchy, black mole** is highly suspicious for **melanoma**, and an excision biopsy provides the most accurate histopathological diagnosis and depth assessment. - This procedure removes the entire lesion with a narrow margin of normal-appearing skin, allowing for comprehensive evaluation of its nature and determining further management. *FNAC of lesion* - **Fine needle aspiration cytology (FNAC)** is generally used for evaluating palpable masses or lymph nodes, not primary skin lesions like a suspicious mole. - It provides only cellular samples, making it difficult to assess architectural features, depth of invasion, or determine definitive malignancy in skin lesions. *Incision biopsy* - An **incision biopsy** involves removing only a partial sample of the lesion, which can lead to sampling error and an inaccurate diagnosis if the most aggressive part is missed. - For suspected melanoma, an incomplete biopsy can compromise subsequent staging and definitive treatment planning. *Wide excision with inguinal lymphadenectomy* - This is an **overly aggressive initial approach** before a definitive diagnosis of melanoma and its stage has been established. - **Wide excision** is typically performed after an excision biopsy confirms melanoma and determines its depth, while **lymphadenectomy** is indicated for confirmed lymph node involvement.
Internal Medicine
3 questionsWhich is the most commonly used chemotherapy regimen in the adjuvant treatment following modified radical mastectomy in the estrogen receptor negative 35 year old female with breast cancer?
Consider the following statements: The clinical features of tension pneumothorax include 1. tracheal shift to contralateral side 2. absent breath sounds on the affected side 3. low output circulatory failure 4. peripheral cyanosis Which of the statements given above is/are correct?
Match List-I with List-II and select the correct answer using the code given below the Lists:
UPSC-CMS 2014 - Internal Medicine UPSC-CMS Practice Questions and MCQs
Question 1: Which is the most commonly used chemotherapy regimen in the adjuvant treatment following modified radical mastectomy in the estrogen receptor negative 35 year old female with breast cancer?
- A. Adriamycin + 5-Fluorouracil
- B. Cyclophosphamide + Adriamycin + 5-Fluorouracil (Correct Answer)
- C. Cyclophosphamide + 5-Fluorouracil
- D. Cyclophosphamide + Methotrexate + 5-Fluorouracil
Explanation: ***Cyclophosphamide + Adriamycin + 5-Fluorouracil*** - The **CAF** (Cyclophosphamide, Adriamycin, 5-Fluorouracil) or **FAC** regimen is a widely used and effective **combination chemotherapy** for adjuvant treatment in **ER-negative breast cancer**, offering a robust approach to systemic control. - This regimen addresses the aggressive nature of **ER-negative tumors**, for which **endocrine therapy** is not an option, and aims to eradicate micrometastases reducing recurrence risk. *Adriamycin + 5-Fluorouracil* - While both **Adriamycin** and **5-Fluorouracil** are active agents in breast cancer, this two-drug combination in isolation is generally considered less potent than multi-agent regimens, particularly for **ER-negative disease**. - It lacks the additional mechanism of action and efficacy provided by **cyclophosphamide**, which is a key component in many standard regimens for this aggressive tumor subtype. *Cyclophosphamide + 5-Fluorouracil* - This two-drug regimen is not a standard frontline or the most common adjuvant chemotherapy for ER-negative breast cancer due to its relatively lower efficacy compared to regimens that include an **anthracycline** like Adriamycin. - The absence of an **anthracycline** like Adriamycin, which is a powerful agent against breast cancer, limits its overall effectiveness in a setting where aggressive systemic treatment is crucial. *Cyclophosphamide + Methotrexate + 5-Fluorouracil* - The **CMF** (Cyclophosphamide, Methotrexate, 5-Fluorouracil) regimen was historically a foundational adjuvant therapy; however, for **ER-negative breast cancer**, regimens containing an **anthracycline** like Adriamycin are generally preferred due to their superior efficacy. - While effective, **CMF** is often considered less potent than anthracycline-containing regimens like **CAF/FAC** in treating aggressive, **ER-negative tumors**, which typically benefit from the broader cytotoxic activity of an anthracycline.
Question 2: Consider the following statements: The clinical features of tension pneumothorax include 1. tracheal shift to contralateral side 2. absent breath sounds on the affected side 3. low output circulatory failure 4. peripheral cyanosis Which of the statements given above is/are correct?
- A. 1 and 3 only
- B. 1, 2 and 3 (Correct Answer)
- C. 2 and 4
- D. 1 and 4
Explanation: ***1, 2 and 3*** - **Tracheal deviation to the contralateral side** is a hallmark sign of tension pneumothorax [1], caused by the increasing pressure in the affected hemithorax pushing mediastinal structures away. - **Absent breath sounds on the affected side** result from the complete collapse of the lung and inability of air to enter the pleural space with inspiration [1]. **Low output circulatory failure** occurs due to increased intrathoracic pressure compressing the heart and great vessels, impairing venous return and cardiac output [2]. *1 and 3 only* - While **tracheal shift to the contralateral side** and **low output circulatory failure** [2] are indeed features, this option incorrectly excludes **absent breath sounds on the affected side**, which is a critical clinical finding in tension pneumothorax. - The absence of breath sounds directly reflects the collapsed lung, a primary mechanical consequence of the condition. *2 and 4* - **Absent breath sounds on the affected side** is correct, but **peripheral cyanosis** is not a *primary* or *early* distinguishing feature of tension pneumothorax. While hypoxemia can lead to cyanosis, it's often a late and less specific sign. - This option misses the crucial finding of **tracheal deviation** and the systemic impact of **circulatory failure** [2], which are more direct indicators of the severity and mechanism of tension pneumothorax. *1 and 4* - **Tracheal shift to the contralateral side** is a correct feature. However, **peripheral cyanosis** is a less specific and often later sign compared to the direct mechanical and circulatory effects. - This option incorrectly omits **absent breath sounds on the affected side** and **low output circulatory failure**, both of which are more consistently present and diagnostically important in tension pneumothorax.
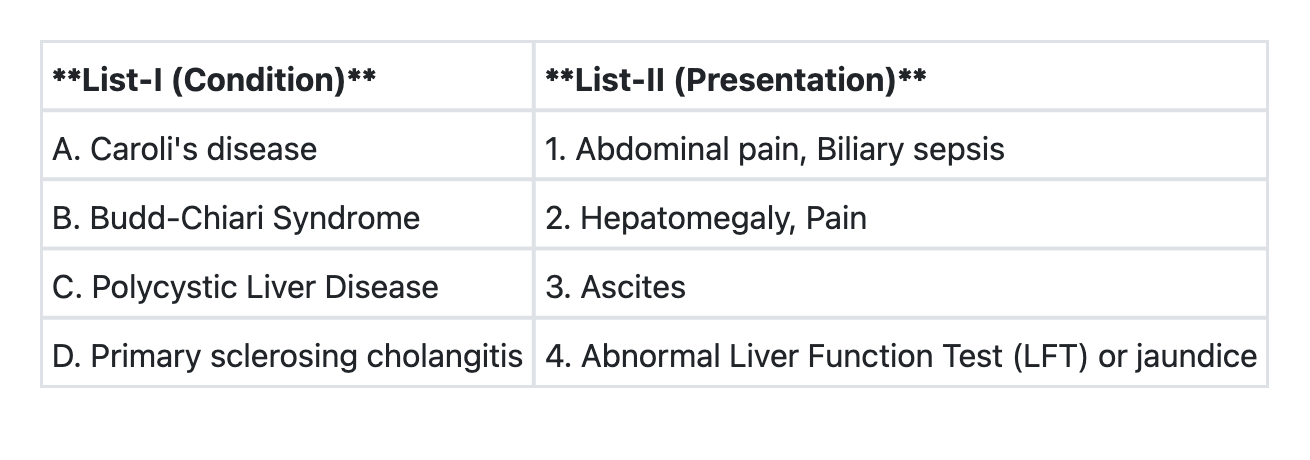
Question 3: Match List-I with List-II and select the correct answer using the code given below the Lists:
- A. A→1 B→3 C→2 D→4 (Correct Answer)
- B. A→1 B→2 C→3 D→4
- C. A→3 B→2 C→4 D→1
- D. A→4 B→3 C→2 D→1
Explanation: ***A→1 B→3 C→2 D→4*** - Caroli's disease is characterized by **dilatation of intrahepatic bile ducts**, predisposing to **bile stasis**, stone formation, and recurrent **biliary sepsis** with associated abdominal pain. - Budd-Chiari Syndrome is defined by **hepatic venous outflow obstruction**, leading to symptoms like **ascites**, hepatomegaly, and abdominal pain. - Polycystic Liver Disease involves the presence of **multiple cysts in the liver**, which can cause **hepatomegaly** and **pain** due to the size and mass effect of the cysts. - Primary sclerosing cholangitis (PSC) is a **cholestatic liver disease** causing inflammation and fibrosis of the bile ducts, leading to **abnormal liver function tests** (elevated alkaline phosphatase and bilirubin) and often presenting with **jaundice**. *A→1 B→2 C→3 D→4* - This option incorrectly matches Budd-Chiari Syndrome with Hepatomegaly, Pain and Polycystic Liver Disease with Ascites. - The hallmark of Budd-Chiari is venous outflow obstruction leading to **ascites**, while **hepatomegaly and pain** are more characteristic symptoms of Polycystic Liver Disease due to the expanding cysts. *A→3 B→2 C→4 D→1* - This option incorrectly associates Caroli's disease with ascites and Primary Sclerosing Cholangitis with Abdominal pain, Biliary sepsis. - Caroli's disease is primarily characterized by **biliary complications** like cholangitis, not ascites, and ascites is a key feature of Budd-Chiari, not Polycystic Liver Disease. *A→4 B→3 C→2 D→1* - This option incorrectly links Caroli's disease with Abnormal LFT/jaundice generally and Primary Sclerosing Cholangitis with Abdominal pain, Biliary sepsis. - While Caroli's can cause abnormal LFTs and jaundice secondarily to cholangitis, its primary specific presentation involves **recurrent infection (biliary sepsis)**. Primary Sclerosing Cholangitis directly causes **abnormal LFTs and jaundice** due to cholestasis, but it is not commonly associated with abdominal pain and biliary sepsis.
Surgery
6 questionsIndications of TURP for Benign Prostatic Hyperplasia (BPH) include: 1. Urinary flow rate of less than 10 mL/second 2. Residual volume of urine >100 mL 3. Serum level of prostatic specific antigen >10 ng/mL 4. Trabeculated Urinary bladder Select the correct answer using the code given below:
Tongue fixation in a patient with carcinoma tongue is staged as
The following procedures are recommended for palliation in a patient with obstructive jaundice due to unresectable carcinoma of head of pancreas except:
Which of the following are contraindications to salvaging accidentally injured spleen during operation? 1. Labile blood pressure 2. Presence of intraperitoneal infection 3. Pre-existing splenic disease 4. Age below 50 years Select the correct answer using the code given below:
Treatment of choice for annular pancreas is
In a patient of gastric outlet obstruction nutritional support is best delivered by:
UPSC-CMS 2014 - Surgery UPSC-CMS Practice Questions and MCQs
Question 1: Indications of TURP for Benign Prostatic Hyperplasia (BPH) include: 1. Urinary flow rate of less than 10 mL/second 2. Residual volume of urine >100 mL 3. Serum level of prostatic specific antigen >10 ng/mL 4. Trabeculated Urinary bladder Select the correct answer using the code given below:
- A. 2, 3 and 4
- B. 1, 2 and 3
- C. 1, 3 and 4
- D. 1, 2 and 4 (Correct Answer)
Explanation: ***1, 2 and 4*** - Urinary flow rate **< 10 mL/s**, **residual urine volume > 100 mL**, and the presence of a **trabeculated bladder** (indicating chronic bladder outlet obstruction) are all relevant indications for considering TURP in BPH. - These findings collectively suggest significant **obstruction** and potential complications of BPH that may warrant surgical intervention. *2, 3 and 4* - This option incorrectly includes a **PSA level > 10 ng/mL** as an indication for TURP, which is primarily a marker for **prostate cancer screening** and not a direct surgical indication for BPH. - While an elevated PSA might prompt further investigation (e.g., biopsy), it doesn't alone necessitate TURP for BPH symptoms. *1, 2 and 3* - This option also incorrectly includes **PSA level > 10 ng/mL** as an indication for TURP. - The other two points (low flow rate and high residual volume) are appropriate indications, but the inclusion of PSA makes this option incorrect. *1, 3 and 4* - This option includes **PSA level > 10 ng/mL** as an indication for TURP, which is incorrect. - Additionally, it omits **residual urine volume > 100 mL**, which is a significant indicator of obstruction and a common reason for considering TURP.
Question 2: Tongue fixation in a patient with carcinoma tongue is staged as
- A. T1
- B. T2
- C. T3
- D. T4 (Correct Answer)
Explanation: ***T4*** - **Tongue fixation** in carcinoma of the tongue indicates advanced local disease classified as **T4a stage** according to AJCC TNM staging. - This finding suggests invasion of **extrinsic tongue muscles**, which causes loss of tongue mobility and represents moderately advanced local disease. - T4a tumors invade through cortical bone, involve the inferior alveolar nerve, floor of mouth, or skin of face, or in the case of tongue, involve deep extrinsic muscles causing fixation. *T1* - **T1 tumors** are small lesions measuring **≤2 cm** in greatest dimension with **depth of invasion (DOI) ≤5 mm**. - They are superficial without invasion of deep structures or causing any functional impairment like tongue fixation. *T2* - **T2 tumors** measure **≤2 cm with DOI >5 mm and ≤10 mm**, OR **>2 cm but ≤4 cm with DOI ≤10 mm**. - While larger than T1, they do not involve deep extrinsic muscles or cause tongue fixation. *T3* - **T3 tumors** are defined as tumors **>4 cm** OR **any tumor with DOI >10 mm**. - Although T3 indicates larger tumor size and deeper invasion, **tongue fixation** specifically indicates T4a stage due to involvement of extrinsic tongue musculature.
Question 3: The following procedures are recommended for palliation in a patient with obstructive jaundice due to unresectable carcinoma of head of pancreas except:
- A. Cholecystojejunostomy with jejunojejunostomy with gastrojejunostomy
- B. Hepaticojejunostomy with gastrojejunostomy
- C. Choledochoduodenostomy with gastrojejunostomy
- D. Choledochoduodenostomy, gastrojejunostomy with pancreaticojejunostomy (Correct Answer)
Explanation: ***Choledochoduodenostomy, gastrojejunostomy with pancreaticojejunostomy*** - **Pancreaticojejunostomy is NOT indicated** in palliative surgery for unresectable pancreatic cancer. - This procedure is used to anastomose the **pancreatic remnant** after **resection** (as in Whipple procedure), not in bypass operations. - Palliation focuses on **relieving biliary and gastric outlet obstruction** without performing pancreatic anastomosis, making this combination inappropriate for palliative care. *Cholecystojejunostomy with jejunojejunostomy with gastrojejunostomy* - **Cholecystojejunostomy** diverts bile flow from the gallbladder to the jejunum, relieving biliary obstruction when the cystic duct is patent. - **Gastrojejunostomy** relieves gastric outlet obstruction, a common complication of pancreatic head cancer. - This represents a valid **triple bypass** palliative approach. *Hepaticojejunostomy with gastrojejunostomy* - **Hepaticojejunostomy** creates a bypass between the common hepatic duct and the jejunum, effectively relieving biliary obstruction. - **Gastrojejunostomy** manages or prevents gastric outlet obstruction. - This **double bypass** is a standard palliative procedure for unresectable pancreatic head cancer. *Choledochoduodenostomy with gastrojejunostomy* - **Choledochoduodenostomy** directly bypasses the biliary obstruction by connecting the common bile duct to the duodenum. - **Gastrojejunostomy** addresses gastric outlet obstruction from duodenal compression by the tumor. - This **double bypass** is another widely accepted palliative approach.
Question 4: Which of the following are contraindications to salvaging accidentally injured spleen during operation? 1. Labile blood pressure 2. Presence of intraperitoneal infection 3. Pre-existing splenic disease 4. Age below 50 years Select the correct answer using the code given below:
- A. 1, 2 and 3 (Correct Answer)
- B. 1, 3 and 4
- C. 2, 3 and 4
- D. 1, 2 and 4
Explanation: ***1, 2 and 3*** - **Labile blood pressure** (1) indicates ongoing hemodynamic instability, making splenic salvage risky due to the potential for further hemorrhage and the need for immediate control. - **Presence of intraperitoneal infection** (2) makes splenic salvage dangerous as the injured spleen provides a niche for bacterial proliferation, increasing the risk of abscess formation and sepsis. - **Pre-existing splenic disease** (3) such as lymphoma or significant architectural changes, can compromise the spleen's integrity and function, making successful and safe salvage unlikely. *1, 3 and 4* - This option incorrectly includes age below 50 years as a contraindication. **Age below 50 years** (4) is generally not a contraindication to splenic salvage; in fact, younger patients, especially children, often have a greater imperative for splenic preservation due to higher risks of **overwhelming post-splenectomy infection (OPSI)**. - While choices 1 and 3 are correct contraindications, choice 4 is not. *2, 3 and 4* - This option incorrectly includes age below 50 years as a contraindication. **Labile blood pressure** (1) is a critical contraindication but is omitted. - Choices 2 and 3 are valid contraindications, but excluding the crucial factor of hemodynamic instability makes this option incomplete. *1, 2 and 4* - This option correctly identifies **labile blood pressure** (1) and **intraperitoneal infection** (2) as contraindications but incorrectly includes **age below 50 years** (4). - It also omits **pre-existing splenic disease** (3), which is another significant reason to avoid salvage.
Question 5: Treatment of choice for annular pancreas is
- A. Resection
- B. Pyloromyotomy
- C. Gastrojejunostomy
- D. Duodenoduodenostomy (Correct Answer)
Explanation: ***Duodenoduodenostomy*** - This procedure bypasses the **annular pancreatic constriction** by creating an anastomosis between two healthy segments of the **duodenum**, restoring normal flow. - It's preferred because it avoids manipulation or resection of the pancreatic tissue itself, which can lead to complications such as **pancreatitis** or **fistula formation**. *Resection* - Direct resection of the **annular pancreas** is generally avoided due to the high risk of **pancreatitis**, **fistulae**, and injury to the **biliary duct** or **main pancreatic duct**. - The abnormal pancreatic tissue is often intimately associated with the **duodenal wall**, making its complete removal difficult and dangerous. *Pyloromyotomy* - This procedure involves incising the muscle layer of the **pylorus** and is typically used for conditions like **pyloric stenosis**. - It does not address the obstruction caused by an annular pancreas around the **duodenum**. *Gastrojejunostomy* - This procedure involves creating a connection between the **stomach** and the **jejunum** to bypass a distal duodenal or pyloric obstruction. - While it can relieve gastric outlet obstruction, it does not directly address the obstruction in the **proximal duodenum** caused by an **annular pancreas**.
Question 6: In a patient of gastric outlet obstruction nutritional support is best delivered by:
- A. Enteral nutrition by Ryles tube
- B. Jejunostomy (Correct Answer)
- C. Gastrostomy
- D. Parenteral nutrition
Explanation: ***Jejunostomy*** - In **gastric outlet obstruction**, the stomach cannot empty properly, making gastric feeding routes (like Ryles tube or gastrostomy) ineffective. - A **jejunostomy** allows direct delivery of **enteral nutrition** into the jejunum, bypassing the obstructed stomach and duodenum. *Enteral nutrition by Ryles tube* - A **Ryles tube** delivers nutrition into the stomach, which is obstructed in this condition, leading to **stasis** and **vomiting**. - This method would be ineffective and potentially dangerous due to the inability of gastric contents to pass beyond the obstruction. *Gastrostomy* - A **gastrostomy** involves placing a tube directly into the stomach, which is still part of the obstructed system. - Feeding via gastrostomy would lead to accumulation of feed in the stomach, mimicking the issues with oral feeding or a Ryles tube. *Parenteral nutrition* - **Parenteral nutrition** is a viable option for nutritional support but is generally considered a second-line therapy after **enteral routes** fail or are contraindicated. - **Enteral feeding**, when possible (as with jejunostomy), is preferred due to lower cost, reduced risk of infection, and better maintenance of gut integrity.
About UPSC-CMS 2014 Questions
This page contains 113 questions from the UPSC-CMS 2014 paper, organised across 16 subjects for focused practice. Every question comes with the correct answer and a detailed explanation to help you understand the underlying concept. Subject-wise organisation lets you target specific areas and identify which topics carried the most weight in this particular year.
Practising year-wise papers is essential for understanding how the UPSC-CMS exam evolves — you can spot trending topics, gauge difficulty shifts, and benchmark your readiness against a real paper. To take your preparation further, download the Oncourse app for AI-driven performance insights, spaced repetition of questions you got wrong, and a personalised study plan built around your UPSC-CMS goals.