All (1550)Anatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q1201
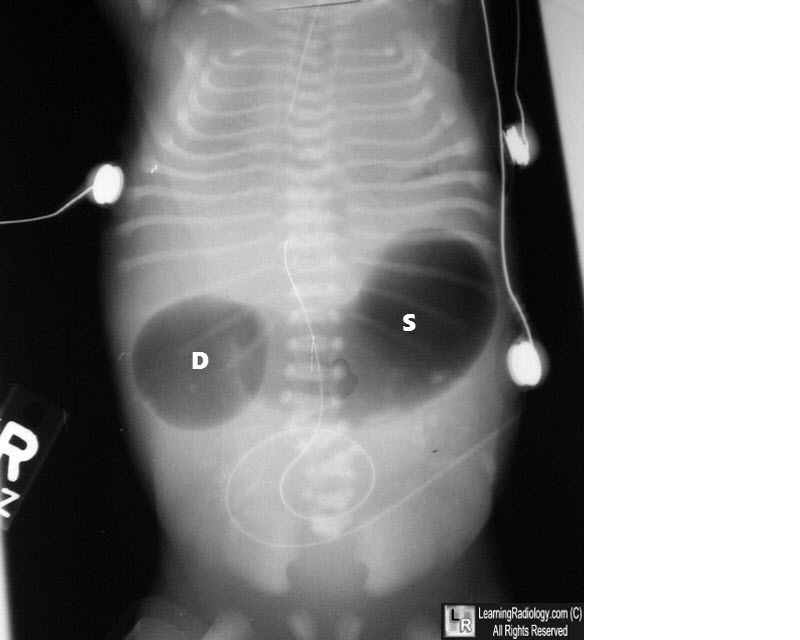
What condition is indicated by the double bubble sign on an abdominal X-ray?
Q1202
Which view is best for visualizing the collapse of the middle lobe of the lung?