All (1550)Anatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q1061
Isolated painful third nerve palsy is a feature of aneurysms of:
Q1062
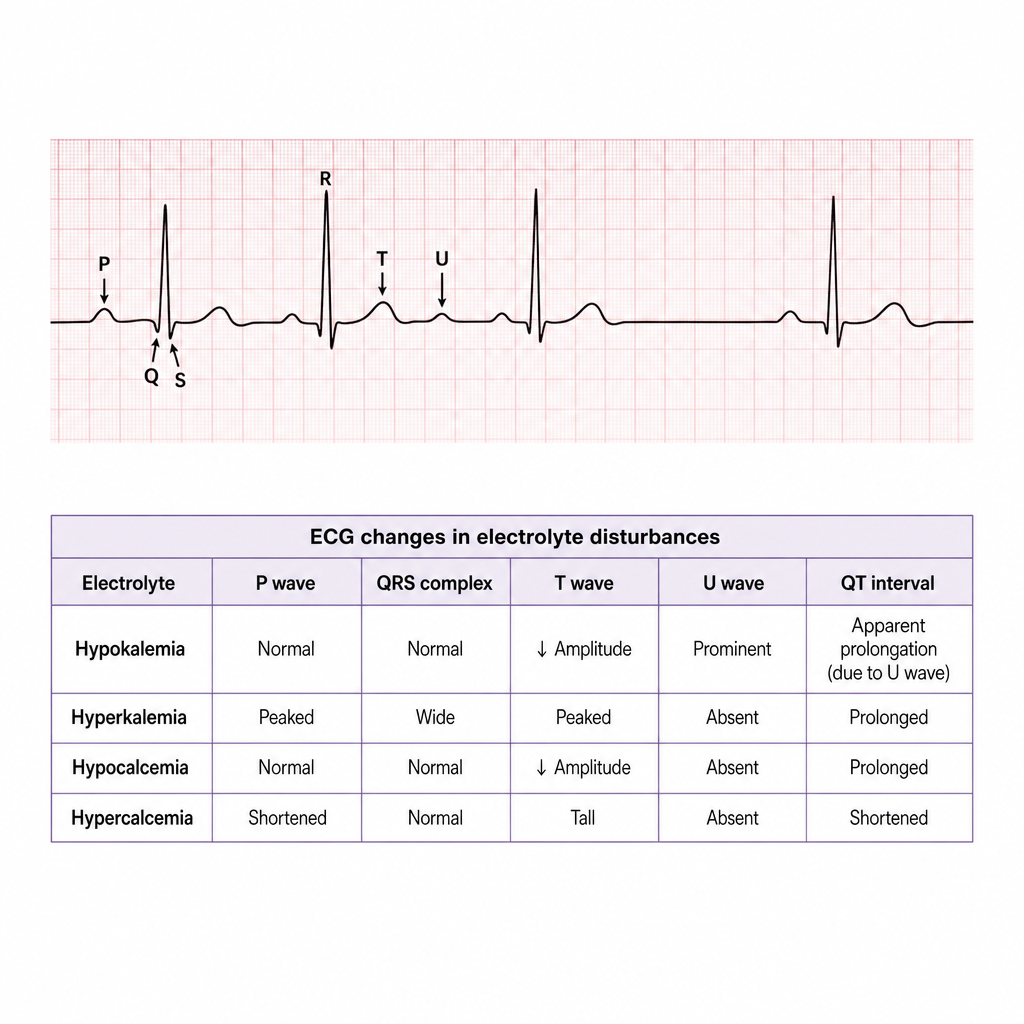
ECG image showing U wave. Patient is on furosemide and beta blocker. What is the most likely diagnosis?
Q1063
In head injury, unilateral dilatation of the pupil is seen due to?