All SubjectsAnatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q51
What is the most common cause of lobar consolidation?
Q52
In head injury, unilateral dilatation of the pupil is seen due to?
Q53
A 68-year-old patient presents with sudden onset of right-sided weakness and slurred speech. The symptoms completely resolve within 30 minutes with no residual neurological deficits. This clinical presentation is most consistent with:
Q54
Impotence is a feature of which of the following:
Q55
In inflammatory myopathy, which group of muscles is not affected
Q56
What is the best immediate management strategy for a patient experiencing respiratory alkalosis due to anxiety-induced hyperventilation?
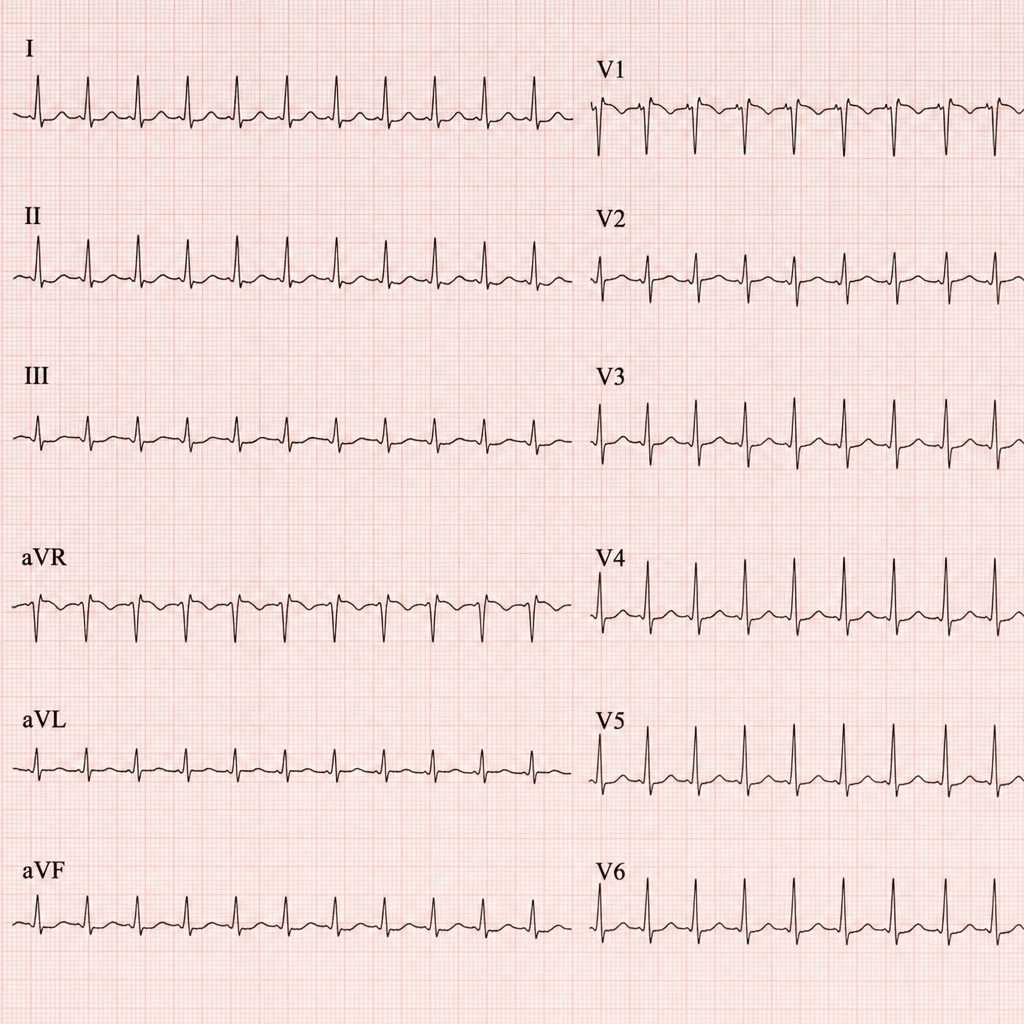
Q57
This patient came to the casualty with palpitations. His ECG has been shown below. What is your diagnosis?
Q58
What is the recommended rate of correction for sodium deficit in patients with chronic hyponatremia?
Q59
A 40-year-old male patient presents to the Emergency department with central chest pain for 2 hours. The ECG shows ST segment depression and cardiac troponins are elevated. The patient has a positive history of previous PCI 3 months back. He is administered Aspirin, Clopidogrel, Nitrates, and LMWH in the Emergency Department and shifted to the coronary care unit. What is the best recommended course of further action?
Q60
Which of the following is not a feature of distal renal tubular acidosis