All SubjectsAnatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q31
What is the drug of choice for bleeding oesophageal varices?
Q32
Treatment of choice for prinzmetal's angina
Q33
Which of the following statements about polio is false?
Q34
Pea soup diarrhea is seen in -
Q35
Which of the following is NOT an indication for a liver biopsy?
Q36
All of the following are features of Obstructive jaundice except:
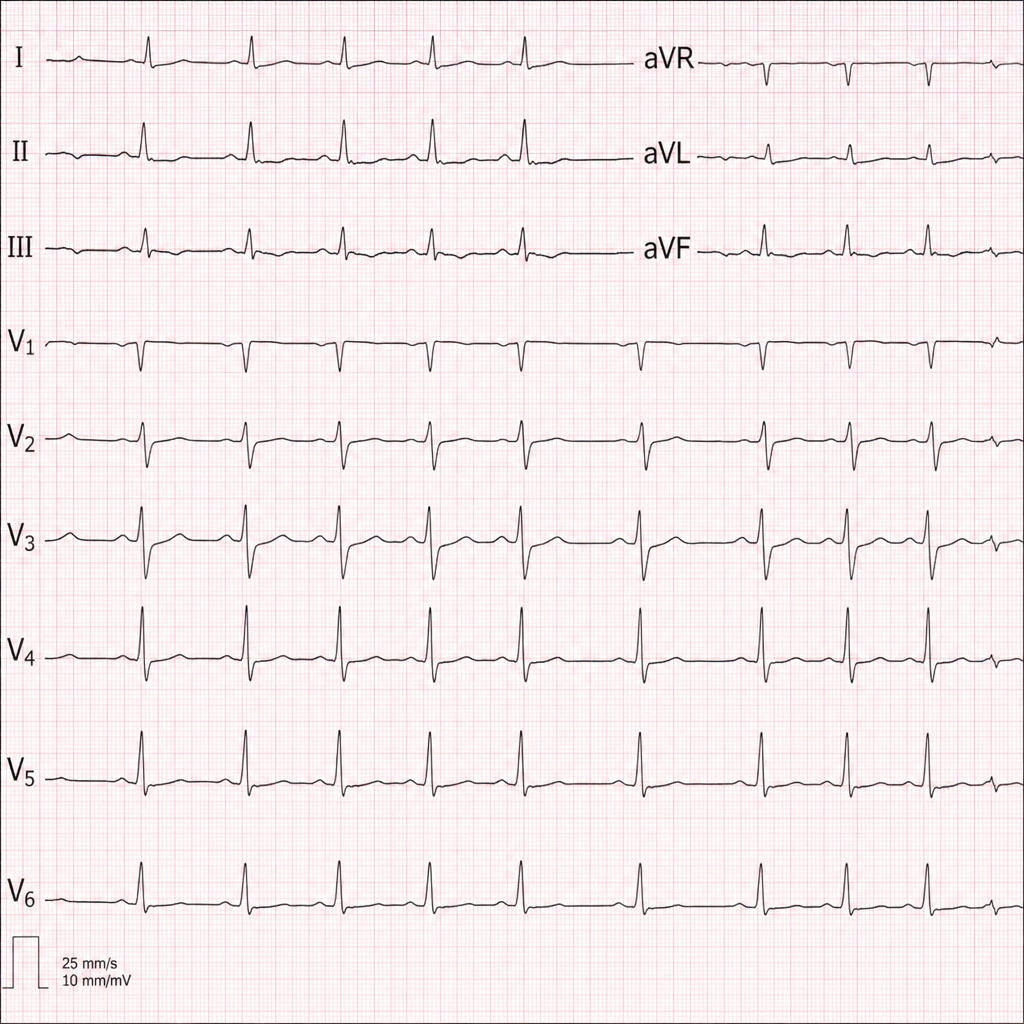
Q37
Diagnose the underlying medical disorder based on the ECG changes.
Q38
A 25 year old female presents with generalized restriction of eye movement in all direction, intermittent ptosis, proximal muscle weakness and fatigability.Which is the MOST useful test in making the diagnosis?
Q39
A 40-year-old male patient presents to the Emergency department with central chest pain for 2 hours. The ECG shows ST segment depression and cardiac troponins are elevated. The patient has a positive history of previous PCI 3 months back. He is administered Aspirin, Clopidogrel, Nitrates, and LMWH in the Emergency Department and shifted to the coronary care unit. What is the best recommended course of further action?
Q40
What is the recommended rate of correction for sodium deficit in patients with chronic hyponatremia?