All SubjectsAnatomy (110)Anesthesiology (34)Biochemistry (129)Community Medicine (109)Dental (16)Dermatology (34)ENT (62)Forensic Medicine (100)General Medicine (2)Internal Medicine (120)Microbiology (108)Obstetrics and Gynecology (79)Ophthalmology (78)Orthopaedics (41)Pathology (90)Pediatrics (33)Pharmacology (134)Physiology (91)Psychiatry (6)Psychiatry (81)Radiology (41)Surgery (52)
Q101
A 40-year-old male with gastroesophageal reflux disease (GERD) is found to have Barrett's esophagus with low-grade dysplasia on endoscopy. What is the most appropriate initial pharmacological treatment for this condition?
Q102
Which of the following is a characteristic finding in distal RTA?
Q103
Which of the following is NOT a feature of Refsum disease?
Q104
All are common sites of primary cancer for bone metastasis except:
Q105
A female patient presents with hirsutism, amenorrhea, and obesity. What is the most likely diagnosis?
Q106
Which of the following is a characteristic feature of Granulomatosis with polyangiitis?
Q107
Match stick test is positive in ?
Q108
In a patient with high clinical suspicion of pulmonary thromboembolism, best investigation would be?
Q109
Wireless capsule endoscopy is done to visualize which of the following condition?
Q110
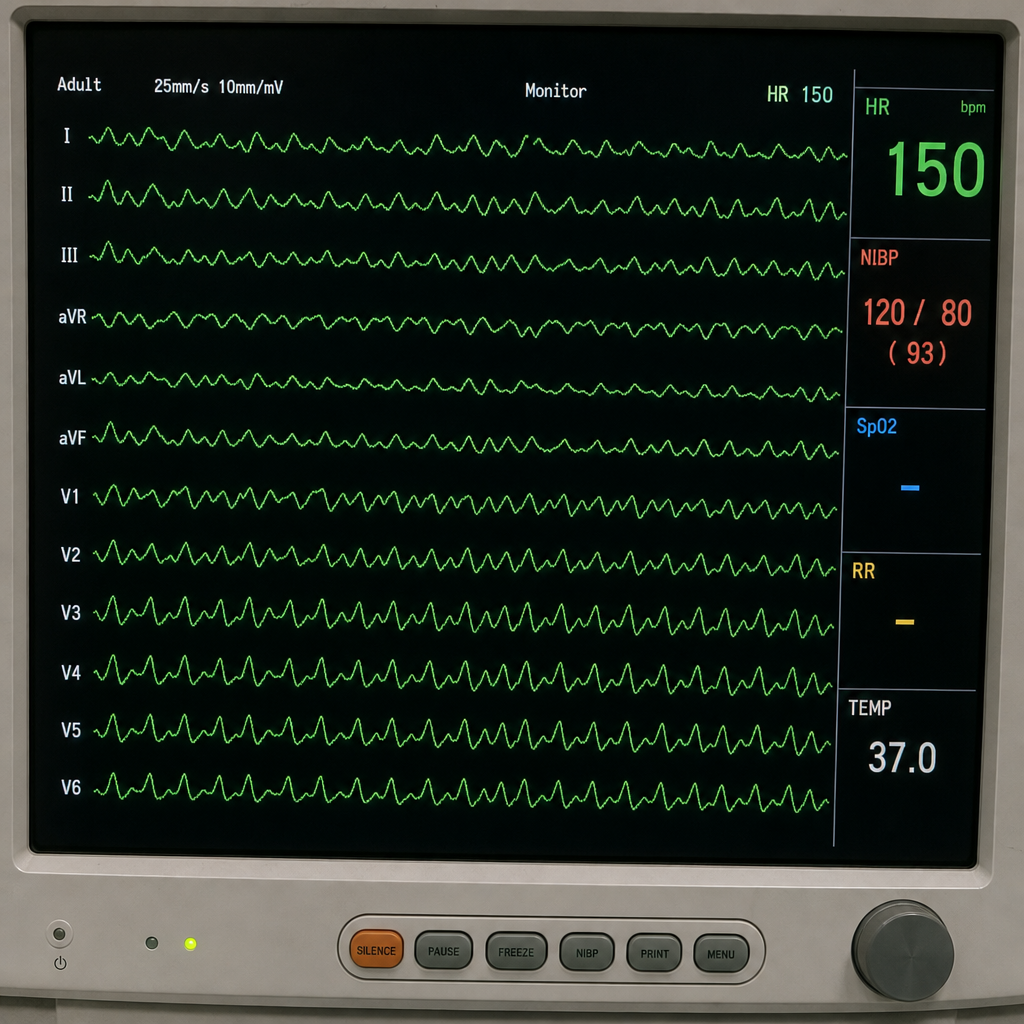
Refer to the provided ECG image. It demonstrates which of the following?