All (70)Anatomy (1)Anatomy (22)Biochemistry (1)Community Medicine (3)Dermatology (4)Forensic Medicine (7)Microbiology (4)Ophthalmology (3)Orthopaedics (4)Pathology (5)Pathology (2)Pediatrics (1)Physiology (2)Psychiatry (1)Radiology (3)Surgery (4)Surgery (3)
Q11
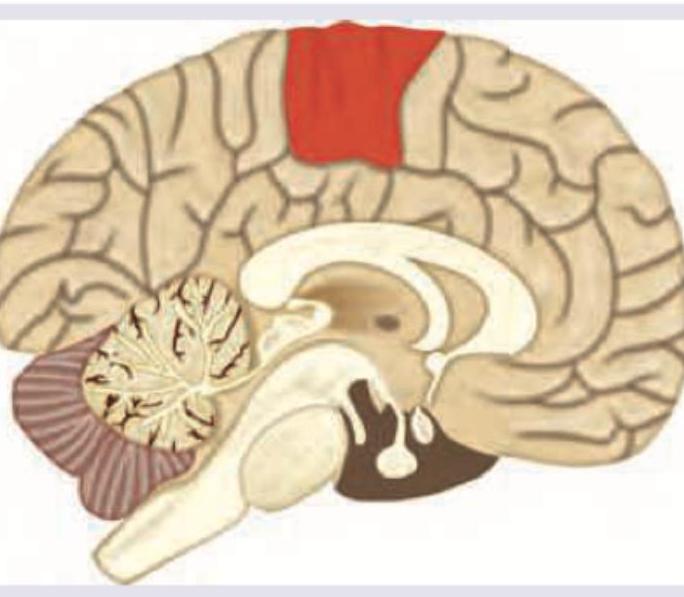
Occlusion of blood supply of the area marked in red will lead to all of the following except: