INI-CET 2018 — Dermatology
5 Previous Year Questions with Answers & Explanations
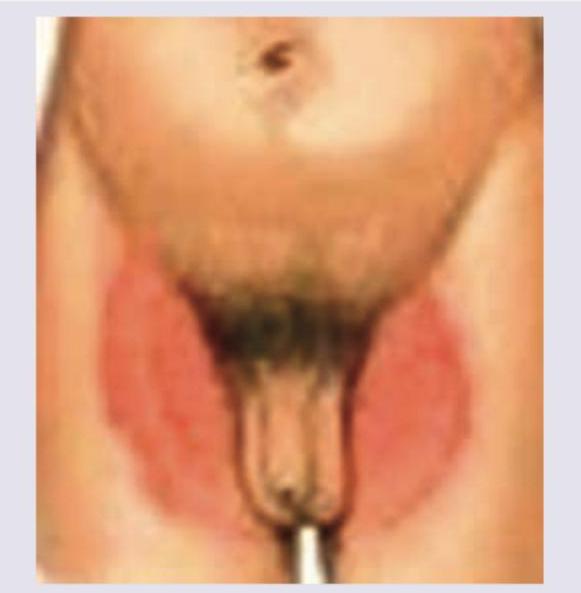
A patient has the following rash in the groin. Which of the following cannot be a cause?
A 28-year-old lady has asymptomatic dome-shaped small lesions on the forehead for the past 2 months. She lives with her 2-year-old daughter who also is having similar lesions. What is the causative agent of these lesions?
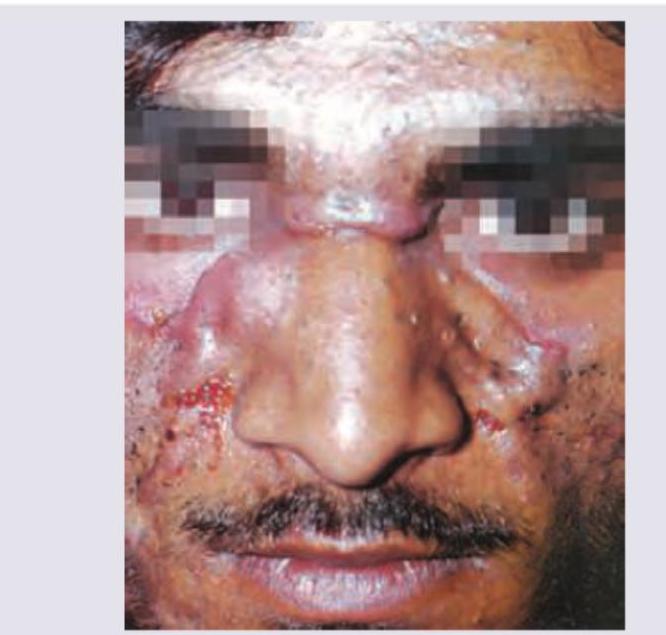
A patient presents with 1-year history of painful nodulocystic acne as shown in the image. Which of the following is the drug of choice for this case?
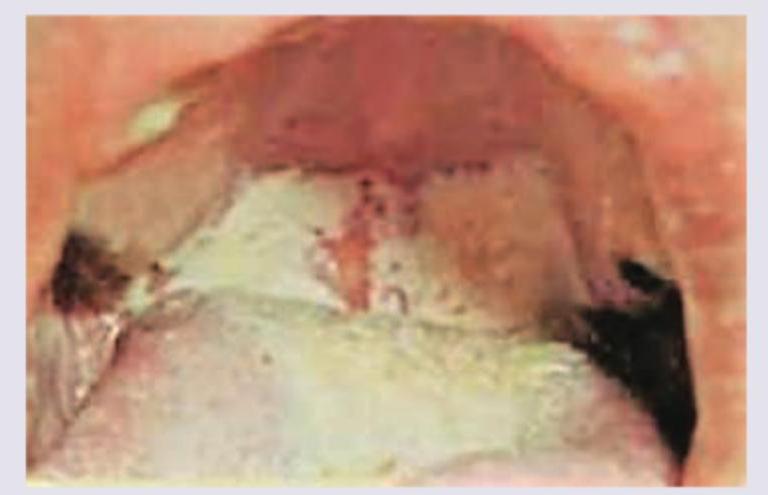
What is the best management of the case shown?
A patient presented with fever and joint pain for which she was put on NSAIDs. After 10 days she developed a skin lesion as shown in the image. Diagnosis is:

INI-CET 2018 - Dermatology INI-CET Practice Questions and MCQs
Question 1: A patient has the following rash in the groin. Which of the following cannot be a cause?
- A. Aspergillus (Correct Answer)
- B. Microsporum
- C. Epidermophyton
- D. Trichophyton
Explanation: ***Aspergillus*** - **Aspergillus** is a **mold (filamentous fungus)**, NOT a dermatophyte, and therefore **cannot cause tinea cruris** (jock itch). - Dermatophytes (Trichophyton, Microsporum, Epidermophyton) are specialized fungi that digest keratin and cause superficial skin infections with characteristic ringworm patterns. - Aspergillus typically causes invasive infections in immunocompromised patients (invasive aspergillosis), allergic bronchopulmonary aspergillosis (ABPA), or rarely deep cutaneous infections in severely immunocompromised individuals—not superficial groin rashes. - **Key distinction:** Tinea cruris = dermatophyte infection; Aspergillus = opportunistic mold *Microsporum* - **Microsporum** species are dermatophytes that CAN cause tinea cruris, though less commonly than Trichophyton and Epidermophyton. - *M. canis* is the most common species, typically causing **tinea capitis** (scalp) and **tinea corporis** (body), but can extend to the groin area. - While not the most frequent cause, it remains a possible etiology and should not be excluded. *Epidermophyton* - **Epidermophyton floccosum** is one of the **most common causes** of tinea cruris. - Presents with itchy, erythematous, scaling patches with well-defined, elevated borders in the inguinal folds. - Thrives in warm, moist environments, making the groin an ideal location. - **Classic presentation:** bilateral involvement with central clearing and advancing scaly borders. *Trichophyton* - **Trichophyton rubrum** is the **MOST common** cause of tinea cruris worldwide, followed by **T. mentagrophytes**. - Causes characteristic pruritic, erythematous, annular or serpiginous lesions with raised, scaly borders. - T. rubrum accounts for the majority of dermatophyte infections in the groin, feet, and nails.
Question 2: A 28-year-old lady has asymptomatic dome-shaped small lesions on the forehead for the past 2 months. She lives with her 2-year-old daughter who also is having similar lesions. What is the causative agent of these lesions?
- A. HSV
- B. HPV
- C. Poxvirus (Correct Answer)
- D. VZV
Explanation: ***Poxvirus*** - The description of asymptomatic, **dome-shaped small lesions** and their presence in both a mother and her young child strongly suggests **molluscum contagiosum**, which is caused by a **poxvirus**. - Molluscum contagiosum lesions are typically **umbilicated**, which often appears dome-shaped, and are highly contagious, commonly spread through close contact. *HSV* - **Herpes Simplex Virus (HSV)** typically causes clusters of **painful vesicles** on an erythematous base, which later crust over. - The lesions described are asymptomatic and dome-shaped, not vesicular or painful. *HPV* - **Human Papillomavirus (HPV)** causes **warts**, which are rough, verrucous papules or plaques, not smooth dome-shaped lesions. - While warts can spread through close contact, their morphology differs significantly from the lesions described. *VZV* - **Varicella-Zoster Virus (VZV)** causes **chickenpox** (widespread itchy vesicles) or **shingles** (painful dermatomal rash). - The lesions described do not fit the characteristic presentation of either chickenpox or shingles, as they are asymptomatic and dome-shaped.
Question 3: A patient presents with 1-year history of painful nodulocystic acne as shown in the image. Which of the following is the drug of choice for this case?
- A. Topical clindamycin
- B. Oral isotretinoin (Correct Answer)
- C. Topical adapalene
- D. Oral doxycycline
Explanation: ***Oral isotretinoin*** - This patient presents with severe **nodulocystic acne**, which is characterized by deep, painful lesions that often lead to scarring, and has been present for 1 year. Oral isotretinoin is the **drug of choice** for severe, recalcitrant nodulocystic acne due to its ability to target all four pathogenic factors of acne. - Isotretinoin reduces **sebum production**, normalizes follicular keratinization, decreases *P. acnes* colonization, and has anti-inflammatory effects, making it highly effective for severe cases. *Topical clindamycin* - **Topical clindamycin** is an antibiotic primarily used for mild to moderate inflammatory acne, particularly papules and pustules. - It is **insufficient** for severe nodulocystic acne due to its limited penetration and inability to address the deeper, more severe inflammation and scarring potential. *Topical adapalene* - **Topical adapalene** is a retinoid used for mild to moderate comedonal and inflammatory acne. It helps normalize follicular keratinization and has anti-inflammatory properties. - While effective for less severe acne, it is generally **not potent enough** to treat severe nodulocystic acne effectively, especially given its chronic nature as described. *Oral doxycycline* - **Oral doxycycline** is a systemic antibiotic used for moderate to severe inflammatory acne, primarily due to its anti-inflammatory properties and its effect on reducing *P. acnes*. - Although it can be used for severe acne, it is **less effective** than oral isotretinoin for nodulocystic acne, especially in the long-term, and does not address the underlying pathogenesis (like sebaceous gland activity) as comprehensively as isotretinoin.
Question 4: What is the best management of the case shown?
- A. Dapsone plus steroids
- B. Stop smoking and screen for cancer (Correct Answer)
- C. Vitamin supplements
- D. Antifungals for oral candidiasis
Explanation: ***Stop smoking and screen for cancer*** - The image shows **smoker's palate (nicotinic stomatitis)**, characterized by diffuse white thickening of the palatal mucosa with red dots representing inflamed salivary gland orifices. This condition is caused by **chronic heat exposure from smoking**. - While generally benign, smoker's palate indicates a high risk for other **oral cancers**, particularly those involving the lips, tongue, and floor of the mouth, necessitating smoking cessation and regular screening. *Dapsone plus steroids* - This combination is typically used for **autoimmune blistering diseases** like **dermatitis herpetiformis** or **pemphigoid**, which present with different clinical features. - Smoker's palate is not an autoimmune condition and would not respond to these treatments. *Vitamin supplements* - Vitamin supplements are not a treatment for smoker's palate, as it is a localized lesion caused by irritation from smoke. - While general nutritional support is good, it doesn't address the underlying cause or potential complications of this specific condition. *Antifungals for oral candidiasis* - **Oral candidiasis (thrush)** typically presents as removable white plaques on the oral mucosa, often associated with immunosuppression or antibiotic use. - The lesions in the image are firmly attached, non-removable, and show specific morphological changes (red dots), which are not characteristic of candidiasis.
Question 5: A patient presented with fever and joint pain for which she was put on NSAIDs. After 10 days she developed a skin lesion as shown in the image. Diagnosis is:
- A. Chikungunya
- B. Dengue
- C. Fixed drug eruption (Correct Answer)
- D. Melasma
Explanation: ***Fixed drug eruption*** - The appearance of a **well-demarcated, erythematous, and pigmented patch** on the skin, combined with a history of recent **NSAID use** and prior fever/arthralgia (suggesting possible prior exposure and sensitization to the drug), is highly characteristic of fixed drug eruption. - FDEs typically recur at the **same site(s)** upon re-exposure to the offending drug, and NSAIDs are known culprits. The lesion often heals with post-inflammatory **hyperpigmentation**. *Chikungunya* - While Chikungunya causes **fever and severe joint pain**, the rash associated with it is typically a more generalized, **maculopapular rash**, not a localized, well-demarcated lesion as seen in the image. - The onset of the skin lesion **10 days after starting NSAIDs** points more towards a drug reaction than a viral exanthem, especially with the appearance of a **pigmented patch**. *Dengue* - Dengue fever presents with **fever, joint pain, and often a rash**, but the rash is usually a generalized **macular or maculopapular eruption**, sometimes with petechiae, and is not typically a single, demarcated, post-inflammatory hyperpigmented lesion. - Similar to Chikungunya, the timing and morphology of the lesion are not typical for Dengue rash. *Melasma* - Melasma is a chronic skin condition causing **dark, discolored patches** on the face, primarily due to hormonal changes (e.g., pregnancy, birth control) or sun exposure. - It does not typically present acutely after drug ingestion with accompanying inflammation or an eruption-like morphology.