Back
USMLE Step 2 CK Pediatrics: High-Yield Topics, Key Presentations and Exam Strategy (2026)
Master USMLE Step 2 CK pediatrics with this comprehensive guide covering high-yield topics, developmental milestones, neonatal emergencies, and age-specific management approaches for 2026.

USMLE Step 2 CK Pediatrics: High-Yield Topics, Key Presentations and Exam Strategy (2026)
You're staring at a 3-year-old with stridor, low-grade fever, and the parents say it started after bedtime. Is it croup? Epiglottitis? Do you examine the throat or not?
Step 2 CK pediatrics isn't about memorizing every childhood disease. It's about rapid pattern recognition: age + symptom cluster = most likely diagnosis + next best step. The exam tests your ability to think like a pediatrician making real-time decisions, not recite textbook facts.
Here's what separates high scorers: they recognize age-based patterns that examiners love, know management decision points that matter, and avoid classic traps that catch 60% of test-takers.
How Step 2 CK Tests Pediatrics
Step 2 CK pediatrics is almost entirely vignette-based. You'll see 15-20 pediatric questions, each presenting a clinical scenario requiring you to:
1. Recognize age-appropriate presentations
2. Identify the most likely diagnosis
3. Choose the next best step in management
The key insight: pediatric presentations are highly age-specific. A 2-month-old with fever gets a full sepsis workup. A 2-year-old with the same fever gets observation if they look well. Age isn't just context — it's the primary diagnostic clue.
Developmental Milestones: The Foundation
Developmental milestones appear in 3-4 questions per exam. Examiners test your ability to recognize normal vs delayed development across four domains:
Key Milestones by Age
Age | Gross Motor | Fine Motor | Language | Social |
|---|---|---|---|---|
2 months | Lifts head prone | Grasps objects | Social smile, coos | Social smile |
6 months | Sits without support | Transfers hand-to-hand | Babbles "ba-ba" | Stranger anxiety |
12 months | Walks independently | Pincer grasp | "Mama/dada" with meaning | Waves bye-bye |
18 months | Runs, kicks ball | Stacks 2-3 blocks | 10-25 words | Uses cup/spoon |
24 months | - | - | 2-word phrases, 50+ words | Parallel play |
Red Flags for Referral
No social smile by 3 months
Not sitting by 9 months
Not walking by 18 months
No words by 16 months
Loss of previously acquired skills (regression)
When memorizing milestone sequences, custom mnemonic chains help lock in the key ages across all four developmental domains that examiners test most frequently.
Practice developmental milestone questions to build pattern recognition for normal vs concerning delays.
Neonatal Emergencies: High-Yield Presentations
Necrotizing Enterocolitis (NEC)
Classic: Premature infant, 1-2 weeks old, feeding intolerance, bloody stools, abdominal distension Key imaging: Pneumatosis intestinalis (gas in bowel wall) on abdominal X-ray Management: NPO, IV antibiotics, surgical consultation if perforation
Respiratory Distress Syndrome (RDS)
Classic: Premature infant <34 weeks, immediate respiratory distress Key findings: Ground-glass appearance on chest X-ray, low surfactant Management: Surfactant replacement, mechanical ventilation
Transient Tachypnea of Newborn (TTN)
Classic: Term infant, C-section delivery, tachypnea within 6 hours Key finding: Fluid in fissures ("wet lung") on chest X-ray Management: Observation — resolves in 24-48 hours Exam trap: Don't confuse TTN with RDS. TTN affects term babies and resolves quickly; RDS affects preemies and requires surfactant.
For comprehensive neonatal scenarios, work through neonatal infection questions that mirror Step 2 CK presentations.
Pediatric Infections: Pattern Recognition
Meningitis: CSF Analysis Patterns
Type | WBC Count | Cell Type | Protein | Glucose |
|---|---|---|---|---|
Bacterial | >1000 | Neutrophils | >100 mg/dL | <40 mg/dL |
Viral | <500 | Lymphocytes | <100 mg/dL | Normal |
Management pearl: Start antibiotics immediately if bacterial suspected. Don't wait for CSF results in ill-appearing children.
Upper Airway Infections
#### Epiglottitis vs Croup
Feature | Epiglottitis | Croup |
|---|---|---|
Fever | High | Low-grade |
Cough | Muffled voice | Barky |
Drooling | Yes | No |
X-ray | Thumb sign | Steeple sign |
Management | Do NOT examine throat | Can examine throat |
When encountering these differential scenarios, Clinical Rounds trains the exact decision-making workflow Step 2 CK tests — presenting age-specific cases and building pattern recognition for "symptom cluster + next best step" combinations.
RSV Bronchiolitis
Peak age: 2-6 months Classic: URI symptoms progressing to wheezing, increased work of breathing Management: Supportive care only — no albuterol, no antibiotics, no steroids Hospitalization criteria: Poor feeding, dehydration, hypoxia
Use pediatric respiratory infection practice questions to master age-based patterns examiners test.
Fluid Management: Holliday-Segar Method
Dehydration questions are guaranteed on Step 2 CK. Master this formula:
Daily Fluid Requirements
First 10 kg: 100 mL/kg/day
Next 10 kg: 50 mL/kg/day
Each kg >20: 20 mL/kg/day
Dehydration Grading
Mild (5%): Dry mucous membranes, decreased tears
Moderate (10%): Sunken eyes, decreased skin turgor
Severe (15%): Sunken fontanelle, poor perfusion, altered mental status
Management: Mild gets oral rehydration. Moderate to severe gets IV fluids.
High-Yield Hematology and Cardiology
Idiopathic Thrombocytopenic Purpura (ITP)
Classic: Previously healthy child, acute petechiae/bruising, platelet count <100,000 Key concept: Diagnosis of exclusion — CBC shows isolated thrombocytopenia Management:
Treat: Platelet count <20,000 OR active bleeding
Observe: Platelet count >20,000 with no serious bleeding
Don't: Give platelet transfusions (destroyed immediately)
Kawasaki Disease
Diagnostic criteria: Fever ≥5 days PLUS 4 of 5:
1. Bilateral conjunctival injection
2. Oral mucosa changes (strawberry tongue, red lips)
3. Cervical lymphadenopathy >1.5 cm
4. Polymorphous rash
5. Extremity changes (edema, erythema, desquamation)
Management: IVIG + high-dose aspirin within 10 days Exam trap: Don't confuse with scarlet fever (sandpaper rash, responds to antibiotics) or viral exanthems (no mucosal involvement).
Study Kawasaki disease presentations to master diagnostic criteria.
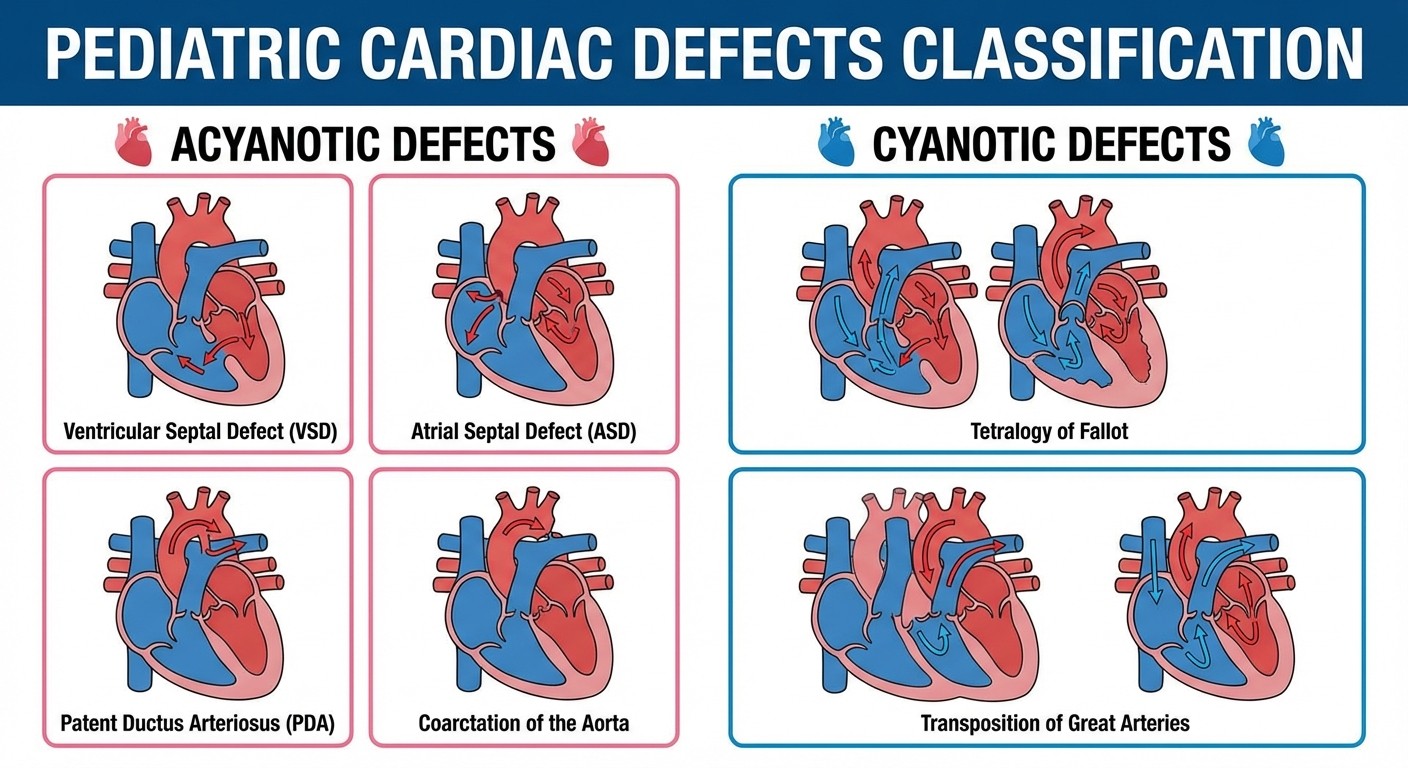
Congenital Heart Disease
Memory trick: The "T"s are cyanotic — Tetralogy, Transposition Acyanotic (Left-to-Right Shunt):
VSD: Most common. Holosystolic murmur
ASD: Fixed split S2
PDA: Continuous "machinery" murmur
Coarctation: Upper extremity hypertension, weak femoral pulses
Cyanotic (Right-to-Left Shunt):
Tetralogy of Fallot: Most common cyanotic defect. Tet spells with crying
Transposition: Aorta and pulmonary artery switched
Age-Based Fever Management
This is the most tested concept in pediatric emergency medicine:
Age Group | Fever Approach | Workup | Disposition |
|---|---|---|---|
0-28 days | Any fever | Full sepsis workup + antibiotics | Hospitalize |
1-3 months | Well-appearing | Blood/urine cultures | Usually hospitalize |
1-3 months | Ill-appearing | Full sepsis workup + antibiotics | Hospitalize |
>3 months | Well-appearing | Supportive care | Home with follow-up |
>3 months | Ill-appearing | Blood culture, consider antibiotics | Case-by-case |
Key insight: The younger the child, the more aggressive the workup. Age 3 months is the critical cutoff.
Child Abuse Recognition
Physical Abuse Red Flags
Multiple fractures in different stages of healing
Posterior rib fractures (high specificity for abuse)
Metaphyseal corner fractures in infants
Bruising in non-mobile infants (<6 months)
Retinal hemorrhages (shaken baby syndrome)
Concerning Patterns
Burns with clear demarcation lines
Bruises over soft tissue areas (cheeks, neck, buttocks)
Injuries inconsistent with developmental abilities
Management: Mandatory reporting to child protective services. Document carefully, obtain skeletal survey in children <2 years.
Vaccine Schedule High-Yields
Focus on timing and contraindications:
Critical Timing
Hepatitis B: Birth, 1-2 months, 6-18 months
DTaP: 2, 4, 6, 15-18 months, 4-6 years
MMR: 12-15 months, 4-6 years
Varicella: 12-15 months, 4-6 years
Key Contraindications
MMR: Pregnancy, immunocompromised (egg allergy is NOT a contraindication — common trap)
Rotavirus: Don't give after 8 months (intussusception risk)
Live vaccines (MMR, varicella, rotavirus): Contraindicated in immunocompromised
Study Strategy
Focus on Age-Specific Patterns
Organize learning by age groups:
Neonates (0-28 days): Congenital anomalies, infections
Infants (1-12 months): Milestones, vaccines, RSV
Toddlers (1-3 years): Developmental delays, croup, Kawasaki
School age (4-12 years): ALL, rheumatic fever
Master "Next Best Step" Logic
1. Stabilize (ABCs if unstable) 2. Diagnose (what test confirms?) 3. Treat (specific intervention)
When you miss questions, Explanation Chat breaks down not just why answers are right, but the underlying pathophysiology and management algorithms — turning mistakes into learning opportunities.
Use Spaced Repetition
Pediatrics has enormous fact density. Use pediatric flashcards to lock in specific ages and numbers.
Frequently Asked Questions
What percentage of Step 2 CK is pediatrics?
Approximately 8-12% of questions, roughly 15-20 questions per exam.
Do I need to memorize growth charts?
No. Focus on recognizing failure to thrive (crossing 2 percentile lines downward) and when growth patterns suggest pathology.
How detailed should vaccine knowledge be?
Know basic timing for DTaP, MMR, Hep B, and rotavirus. Understand live vs inactivated vaccines and contraindications. Don't memorize every vaccine.
Should I study rare genetic syndromes?
Focus on common presentations of common diseases. Step 2 CK tests bread-and-butter pediatrics, not zebra diagnoses.
How do I approach milestone questions?
Learn key ages for major milestones. Focus on red flags requiring referral rather than memorizing every milestone.
What's the best way to distinguish similar conditions?
Create comparison tables for common differentials. Focus on 1-2 key distinguishing features rather than memorizing everything.
---
Pediatrics on Step 2 CK is about pattern recognition and age-appropriate management. Focus on high-yield presentations, master age-based approaches to common symptoms, and practice clinical decision-making that mirrors real pediatric practice.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.