
Neonatal infections — MCQs

On this page
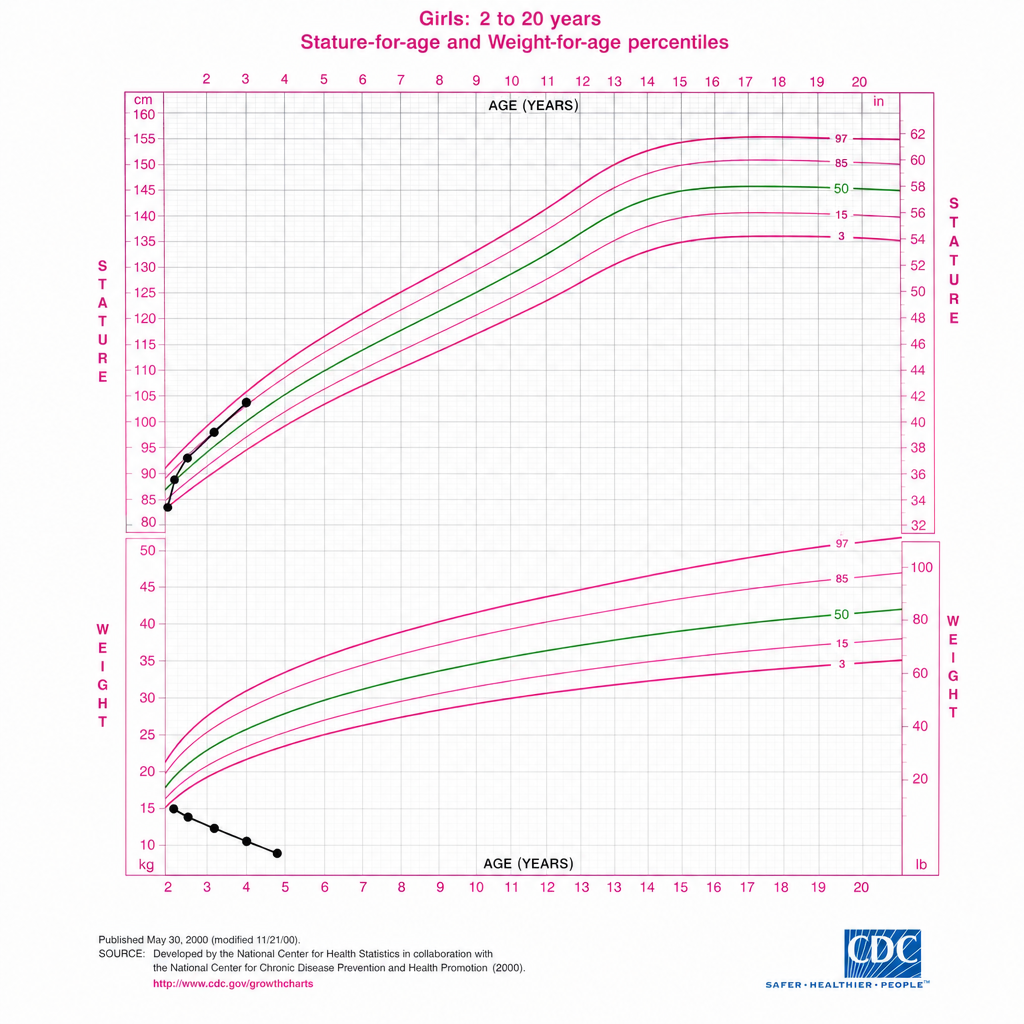
A 4-year-old girl is brought to the clinic for a well-child visit. Her growth chart is shown. She was born at term with a birth weight of 3.4 kg. Her weight at 12 months was at the 50th percentile, at 24 months at the 25th percentile, and today her weight plots below the 3rd percentile. Her length has followed the 25th percentile consistently. Her parents report she has had three to four loose, foul-smelling, greasy stools per day since she began eating gluten-containing foods at 12 months. Laboratory studies show hemoglobin 9.8 g/dL with microcytic anemia, albumin 2.8 g/dL, and zinc level below normal. Anti-tissue transglutaminase IgA antibodies are elevated. Which of the following is the most likely primary etiology of her growth pattern?
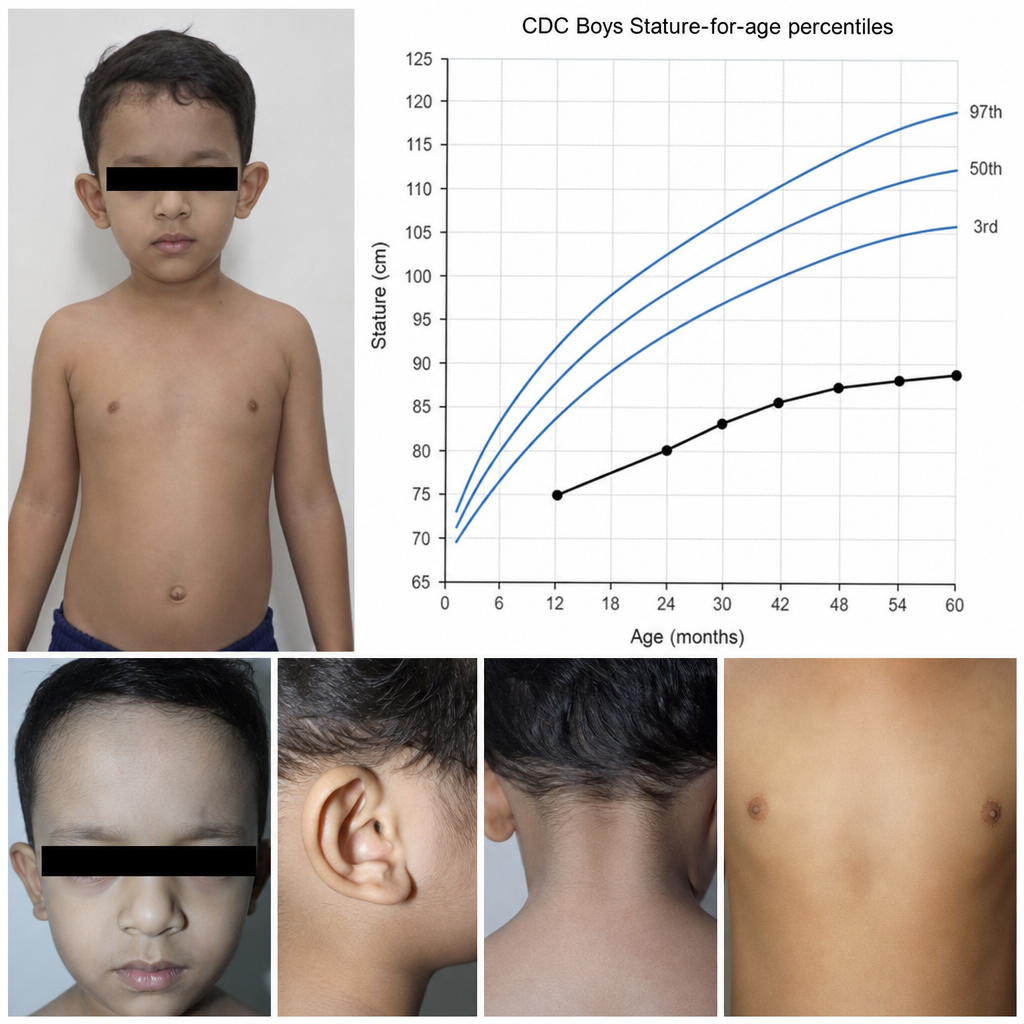
A 3-year-old boy is referred for evaluation of short stature and dysmorphic features. The growth chart image provided shows his height consistently tracking below the 3rd percentile since 12 months of age with normal head circumference. On examination he has a broad forehead, hypertelorism, low-set posteriorly rotated ears, a webbed neck, widely spaced nipples, and a harsh systolic murmur loudest at the left upper sternal border. Karyotype returns as 46,XY. Which of the following additional findings would most strongly support the unifying diagnosis in this child?
Vitamin K supplementation is given to neonates to prevent _____ .
A mother delivers in a rural area under the guidance of a skilled care attendant. Which of the following statements is incorrect regarding the care provided by the skilled care attendant at birth?
A baby presents with hydrocephalus, intracranial calcifications, and chorioretinitis. What is the most probable diagnosis?
Practice by Chapter
Early-onset sepsis
Practice Questions
Late-onset sepsis
Practice Questions
Group B streptococcal disease
Practice Questions
Neonatal meningitis
Practice Questions
Congenital TORCH infections
Practice Questions
Neonatal HSV
Practice Questions
Neonatal candidiasis
Practice Questions
Necrotizing enterocolitis
Practice Questions
Omphalitis
Practice Questions
Nursery outbreaks
Practice Questions
Antibiotic stewardship in NICU
Practice Questions
Diagnostic approach to neonatal sepsis
Practice Questions
Maternal factors and neonatal infection risk
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app