Back
How to Study Neurology for USMLE Step 1 2026: High-Yield Brain Anatomy, Pathways, Classic Diseases and Exam Strategy
Master USMLE Step 1 neurology with this comprehensive guide to high-yield brain anatomy, spinal cord pathways, classic diseases, and proven study strategies for 2026.
How to Study Neurology for USMLE Step 1 2026: High-Yield Brain Anatomy, Pathways, Classic Diseases and Exam Strategy
You are probably staring at a 2,000-page neurology textbook right now, wondering how anyone memorizes every single pathway, tract, and syndrome for Step 1. Here's what changed everything for me: Step 1 neurology isnt clinical neurology. Its pattern recognition built on precise anatomical knowledge.
USMLE Step 1 has roughly 30-40 neurology questions. Each one tests the same fundamental skill: given a symptom pattern, can you localize the lesion? Can you trace the disrupted pathway? Can you name the classic syndrome that results?
The students who crush neurology dont memorize 500 diseases. They master 15 core anatomical concepts so well they can derive the answer from first principles. Lesion in the left frontal lobe? Broca aphasia. Hemisection at T10? Brown-Séquard syndrome with ipsilateral motor loss and contralateral pain loss.
This guide teaches you exactly how to approach Step 1 neurology: anatomical precision first, pathway tracing second, syndrome recognition third. By the end, you'll think like the test makers.
Understanding Step 1 Neurology: Anatomy-Based Pattern Recognition
Step 1 neurology questions follow a predictable format. You get a vignette describing specific neurological deficits, and you must identify either the lesion location, the affected pathway, or the resulting syndrome.
The key insight: every neurological symptom has an anatomical basis. Loss of fine touch but preserved pain sensation? Dorsal column lesion. Face weakness sparing the forehead? Upper motor neuron CN VII lesion. Choreiform movements with personality changes? Huntington disease affecting the caudate nucleus.
Master the anatomy-symptom relationships for 15 core structures, and you can answer 80% of Step 1 neurology questions without memorizing hundreds of rare syndromes.
The Step 1 Neurology Framework
Level 1: Localize the lesion - Which anatomical structure is damaged? Level 2: Identify the pathway - Which tract or neural circuit is disrupted? Level 3: Name the syndrome - What classic pattern results from this lesion?
This systematic approach works because Step 1 tests fundamental mechanisms, not rare clinical presentations. A Brown-Séquard syndrome question tests whether you understand spinal cord anatomy, not whether you've seen 20 patients with spinal cord hemisection.
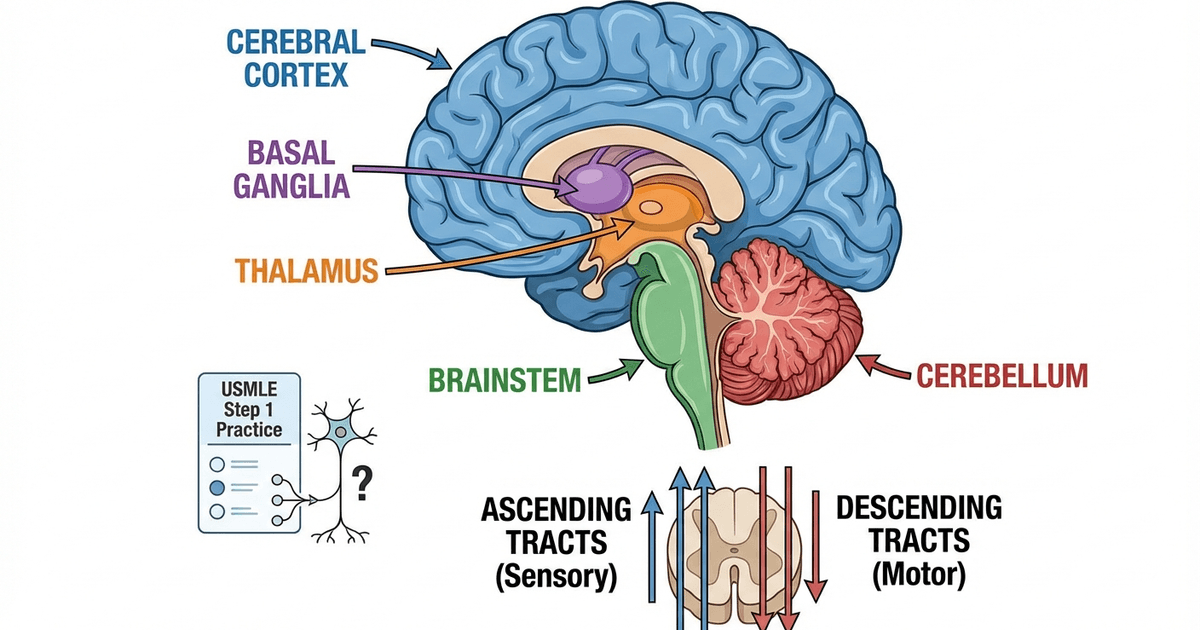
High-Yield Brain Anatomy: Core Structures and Functions
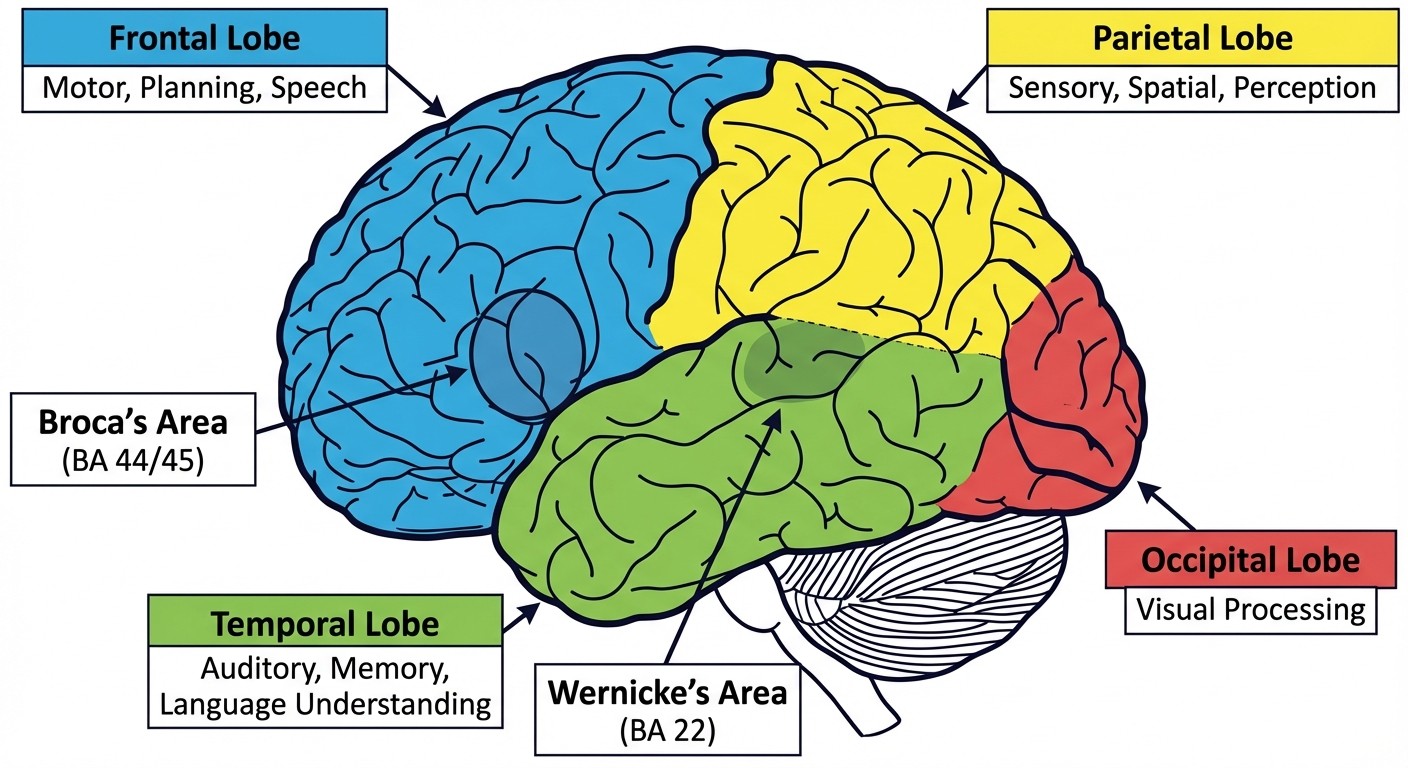
Cerebral Cortex and Language Areas
The frontal, parietal, temporal, and occipital lobes each have specific functions that appear repeatedly on Step 1. Focus on these high-yield correlations:
Frontal lobe: Motor cortex, Broca area (BA 44/45 in dominant hemisphere), executive function. Lesions cause contralateral motor weakness, Broca aphasia (non-fluent speech with intact comprehension), or personality changes. Parietal lobe: Sensory cortex, spatial awareness, dominant hemisphere language processing. Lesions cause contralateral sensory loss, neglect syndrome (non-dominant), or Gerstmann syndrome (dominant). Temporal lobe: Wernicke area (BA 22 in dominant hemisphere), hippocampus, primary auditory cortex. Lesions cause Wernicke aphasia (fluent but meaningless speech), memory impairment, or auditory processing deficits. Occipital lobe: Primary visual cortex. Lesions cause contralateral homonymous hemianopia with macular sparing.
The language areas deserve special attention. Broca area controls speech production - damage causes non-fluent aphasia where patients understand everything but cant speak fluently. Wernicke area processes language comprehension - damage causes fluent but meaningless speech. Both are typically located in the dominant (usually left) hemisphere.
Basal Ganglia Circuit: Movement Control
The basal ganglia circuit controls voluntary movement through two competing pathways: direct (facilitates movement) and indirect (inhibits movement). Understanding this circuit explains multiple Step 1 diseases.
Direct pathway: Cortex → striatum → GPi/SNr → thalamus → cortex. This pathway facilitates movement. Dopamine from the substantia nigra activates D1 receptors, promoting this "go" signal. Indirect pathway: Cortex → striatum → GPe → STN → GPi/SNr → thalamus → cortex. This pathway inhibits movement. Dopamine activates D2 receptors, reducing this "stop" signal. Clinical correlations: In Parkinson disease, dopamine loss reduces activation of both pathways, but the net effect favors the indirect pathway, causing bradykinesia and rigidity. In Huntington disease, GABAergic neurons in the striatum degenerate, disrupting both pathways and causing choreiform movements.
When I was studying the basal ganglia, Oncourse AI's mnemonic generator created this memorable framework: "Direct = Dopamine helps you Dance, Indirect = Inhibits, so when dopamine's gone you're slow." Simple visual associations like this lock in complex circuitry far better than rereading textbook diagrams.
Cerebellum: Movement Coordination
The cerebellum coordinates movement and maintains balance through distinct functional regions:
Cerebellar hemispheres: Control ipsilateral limb coordination. Lesions cause limb ataxia, intention tremor, and dysmetria on the same side as the lesion. Vermis: Controls trunk stability and gait. Lesions cause truncal ataxia and wide-based gait without significant limb involvement. Flocculonodular lobe: Controls balance and eye movements. Lesions cause nystagmus and balance problems.
Key point for Step 1: cerebellar lesions cause ipsilateral symptoms, unlike most brain lesions which cause contralateral deficits. This is because cerebellar efferents cross twice, canceling out the crossing.
Brainstem Anatomy: Cranial Nerve Levels
Memorize which cranial nerves originate at each brainstem level - this appears on every Step 1 exam:
Midbrain: CN III (oculomotor), CN IV (trochlear) Pons: CN V (trigeminal), CN VI (abducens), CN VII (facial), CN VIII (vestibulocochlear) Medulla: CN IX (glossopharyngeal), CN X (vagus), CN XI (spinal accessory), CN XII (hypoglossal)
Understanding brainstem organization helps you localize lesions from cranial nerve deficits. Multiple cranial nerve palsies at the same level suggest a brainstem lesion rather than individual nerve problems.
Spinal Cord Tracts: Pathway Anatomy and Clinical Syndromes
Major Ascending and Descending Tracts
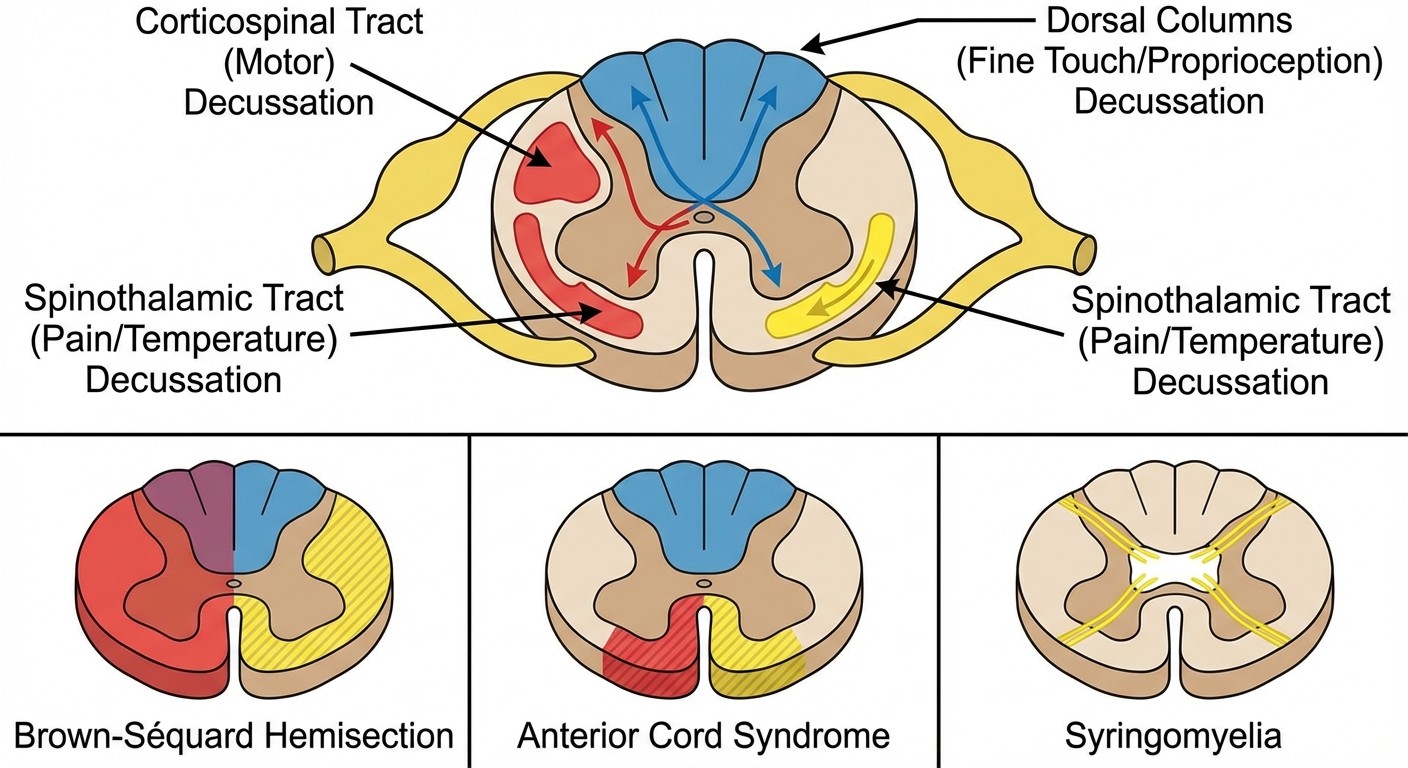
Corticospinal tract (descending): Carries motor commands from motor cortex to spinal motor neurons. Decussates at the pyramids in the medulla. Upper motor neuron lesions cause spasticity, hyperreflexia, and Babinski sign. Dorsal columns (ascending): Carry fine touch, vibration, and proprioception. Fibers travel ipsilaterally in the spinal cord and decussate in the medulla at the nucleus gracilis/cuneatus. Include fasciculus gracilis (legs) and fasciculus cuneatus (arms). Spinothalamic tract (ascending): Carries pain and temperature sensation. Fibers cross within 1-2 levels of entry in the anterior white commissure, then ascend contralaterally to the thalamus.
The crossing patterns are crucial for Step 1. Dorsal columns cross in the medulla, so spinal cord lesions cause ipsilateral loss of fine touch/proprioception. Spinothalamic fibers cross immediately, so spinal cord lesions cause contralateral loss of pain/temperature sensation.
Classic Spinal Cord Syndromes
Understanding these syndromes requires precise knowledge of tract anatomy:
Brown-Séquard syndrome (hemisection):
Ipsilateral: UMN weakness (corticospinal), loss of fine touch/proprioception (dorsal columns)
Contralateral: Loss of pain/temperature (spinothalamic)
Cause: penetrating trauma, tumor
Anterior cord syndrome:
Bilateral: UMN weakness, loss of pain/temperature
Preserved: Fine touch/proprioception (dorsal columns spared)
Cause: anterior spinal artery infarct
Syringomyelia:
Cape distribution loss of pain/temperature (crossing fibers in anterior commissure affected)
Preserved: Fine touch, motor function initially
Associated with Chiari malformations
Subacute combined degeneration:
Bilateral: Loss of proprioception/vibration (dorsal columns) + UMN signs (lateral corticospinal)
Cause: vitamin B12 deficiency
Progression: sensory symptoms first, then motor
Here's how I approached spinal cord syndromes: instead of memorizing each pattern separately, I used Oncourse's spaced repetition flashcards to drill the anatomical basis. When the system detected I was confusing Brown-Séquard with anterior cord syndrome, it automatically increased exposure to questions contrasting these patterns until the distinction was solid.
Cranial Nerve Pathways: High-Yield Clinical Correlations
CN III (Oculomotor): Surgical vs Medical Palsies
CN III controls most extraocular muscles plus pupillary constriction via parasympathetic fibers. The anatomical arrangement of these fibers creates two distinct clinical patterns:
Surgical CN III palsy: Complete ptosis, "down and out" eye position, MYDRIASIS (dilated pupil). Caused by external compression (posterior communicating artery aneurysm) affecting superficial parasympathetic fibers first. Medical CN III palsy: Same motor findings but PUPIL-SPARING. Caused by ischemia (diabetes, hypertension) affecting the nerve core while sparing superficial parasympathetic fibers.
The pupil response distinguishes these emergent (surgical) from non-emergent (medical) causes.
CN VII (Facial): Upper vs Lower Motor Neuron Lesions
CN VII innervates facial muscles, but the innervation pattern creates distinct lesion patterns:
Upper motor neuron CN VII lesion: Forehead muscles SPARED (bilateral cortical innervation), lower face affected contralaterally. Seen in strokes. Lower motor neuron CN VII lesion: ENTIRE ipsilateral face affected including forehead. Classic example: Bell palsy.
This distinction helps localize lesions above or below the facial nucleus in the pons.
CN VIII (Vestibulocochlear): Acoustic Neuroma Presentation
CN VIII carries hearing and balance information. Acoustic neuromas (vestibular schwannomas) present with a classic triad:
1. Progressive unilateral sensorineural hearing loss
2. Tinnitus
3. Unsteady gait/balance problems
When bilateral, suspect neurofibromatosis type 2 (NF2). The key is gradual onset - sudden hearing loss suggests different pathology.
High-Yield Neurology Diseases: Mechanism-Based Understanding
Multiple Sclerosis: Demyelination Patterns
Multiple sclerosis involves oligodendrocyte destruction leading to CNS demyelination. Step 1 focuses on the pathophysiology and diagnostic criteria:
Pathology: Periventricular white matter plaques, oligodendrocyte loss, inflammatory infiltrates Clinical pattern: Relapsing-remitting course with symptoms separated in time and space Diagnosis: McDonald criteria requiring evidence of CNS lesions disseminated in time and space Classic presentations: Optic neuritis, internuclear ophthalmoplegia (INO), Lhermitte sign
Internuclear ophthalmoplegia deserves special attention. Its caused by a lesion in the medial longitudinal fasciculus (MLF) in the brainstem, causing impaired adduction on the affected side with nystagmus in the abducting eye. In young adults, think MS. In elderly adults, think brainstem stroke.
Amyotrophic Lateral Sclerosis: Motor Neuron Degeneration
ALS affects both upper and lower motor neurons, creating a characteristic pattern:
Upper motor neuron signs: Spasticity, hyperreflexia, Babinski sign Lower motor neuron signs: Muscle atrophy, fasciculations, hyporeflexia Key feature: NO sensory involvement (purely motor disease) Genetics: SOD1 mutations in familial cases
The combination of UMN and LMN signs in the same limb distinguishes ALS from other motor disorders.
Huntington Disease: Basal Ganglia Degeneration
Huntington disease results from CAG trinucleotide repeat expansion causing selective neuronal loss:
Pathology: Caudate nucleus atrophy, loss of GABAergic neurons in striatum Clinical triad: Chorea, cognitive decline, psychiatric symptoms Genetics: CAG repeat expansion in huntingtin gene (chromosome 4) Inheritance: Autosomal dominant with anticipation
The choreiform movements result from disrupted basal ganglia circuits controlling movement initiation and termination.
Alzheimer Disease: Protein Aggregation
Alzheimer disease involves two major protein aggregation pathways:
Amyloid plaques: Extracellular β-amyloid protein deposits Neurofibrillary tangles: Intracellular tau protein aggregates Neurochemical change: Loss of acetylcholine from nucleus basalis of Meynert Clinical progression: Memory impairment → cognitive decline → functional decline
The acetylcholine loss explains why cholinesterase inhibitors provide symptomatic benefit.
Understanding these mechanisms helps when I need clarification on complex pathways. Rezzy AI lets me ask specific questions like "Why does Huntington disease cause chorea but Parkinson causes bradykinesia when both affect the basal ganglia?" The AI explains that its about which specific circuits and neurotransmitters are affected, turning confusing facts into logical consequences of the pathophysiology.
Neuropharmacology: High-Yield Pathways and Mechanisms
Dopamine Pathways: Clinical Significance
Dopamine functions through four major brain pathways, each with distinct clinical relevance:
Mesolimbic pathway: Ventral tegmental area to nucleus accumbens. Mediates reward and motivation. Involved in addiction and schizophrenia positive symptoms. Mesocortical pathway: VTA to prefrontal cortex. Involved in cognition and executive function. Hypofunction contributes to schizophrenia negative symptoms. Nigrostriatal pathway: Substantia nigra to striatum. Controls voluntary movement. Degeneration causes Parkinson disease. Antipsychotic blockade causes extrapyramidal symptoms. Tuberoinfundibular pathway: Hypothalamus to anterior pituitary. Inhibits prolactin release. Antipsychotic blockade causes hyperprolactinemia.
Understanding these pathways explains why antipsychotics cause movement disorders (nigrostriatal blockade) and elevated prolactin (tuberoinfundibular blockade) while treating psychosis (mesolimbic blockade).
GABA System: Inhibitory Mechanisms
GABA is the brain's primary inhibitory neurotransmitter, working through GABA-A (ionotropic) and GABA-B (metabotropic) receptors:
Benzodiazepines: Enhance GABA-A receptor function by increasing chloride channel opening frequency. Cause anxiolysis, sedation, muscle relaxation, and amnesia. Barbiturates: Enhance GABA-A receptors by increasing chloride channel opening duration. More dangerous in overdose due to respiratory depression. Clinical correlation: Both drug classes enhance GABAergic inhibition but through different mechanisms, explaining their similar effects but different safety profiles.
Norepinephrine Pathways: Mood and Arousal
The locus coeruleus in the brainstem provides most brain norepinephrine via widespread projections:
Functions: Arousal, attention, mood regulation, stress response Clinical relevance: Target of many antidepressants (TCAs, SNRIs) Pathology: Degeneration in depression, hyperactivity in anxiety disorders
Congenital and Pediatric Neurology
Chiari Malformations: Hindbrain Abnormalities
Chiari malformations involve displacement of hindbrain structures through the foramen magnum:
Type I: Cerebellar tonsils herniate below foramen magnum. Often asymptomatic until adulthood. May cause syringomyelia. Type II: More severe with brainstem displacement. Always associated with myelomeningocele (spina bifida). Causes hydrocephalus and cranial nerve deficits.
The association between Chiari II and myelomeningocele is universal - if you see one, look for the other.
Neural Tube Defects: Embryological Failures
Neural tube defects result from failed neural tube closure during early embryogenesis:
Spina bifida occulta: Incomplete vertebral arch closure without neural tissue involvement. Often asymptomatic with skin dimple or hair tuft. Meningocele: Meningeal sac protrudes through spinal defect without neural tissue. Better prognosis. Myelomeningocele: Both meninges and spinal cord protrude. Causes neurological deficits below the lesion level. Associated with Chiari II malformation.
Prevention involves periconceptional folic acid supplementation.
Neurofibromatosis: Tumor Syndromes
Two distinct genetic disorders with different tumor patterns:
NF1 (chromosome 17):
Café-au-lait spots (>6 spots >0.5cm)
Neurofibromas (benign peripheral nerve tumors)
Lisch nodules (iris hamartomas)
Optic gliomas
NF2 (chromosome 22):
Bilateral acoustic neuromas (pathognomonic)
Fewer skin manifestations
Meningiomas, schwannomas
The mnemonic "17 = spots, 22 = bilateral acoustic neuromas" helps distinguish these conditions.
Vascular Neurology: Stroke Syndromes and Anatomy
Circle of Willis and Vascular Territories
Understanding cerebral blood supply helps predict stroke syndromes:
Anterior circulation: Internal carotid → anterior cerebral artery (ACA), middle cerebral artery (MCA) Posterior circulation: Vertebral arteries → basilar artery → posterior cerebral artery (PCA) MCA stroke: Contralateral face and arm weakness greater than leg, aphasia if dominant hemisphere, neglect if non-dominant hemisphere ACA stroke: Contralateral leg weakness greater than face/arm, personality changes PCA stroke: Contralateral homonymous hemianopia with macular sparing
Posterior Circulation Strokes
PICA (lateral medullary/Wallenberg syndrome):
Ipsilateral: Facial pain/temperature loss, Horner syndrome, ataxia
Contralateral: Body pain/temperature loss
Crossed symptoms: Dysphagia, hoarseness (CN IX/X)
Basilar artery stroke: Can cause "locked-in syndrome" - preserved consciousness with quadriplegia and inability to speak
Watershed Infarcts
Watershed areas between vascular territories are vulnerable during hypotension:
"Man in a barrel" syndrome: Proximal arm weakness with spared distal muscles, occurs in watershed areas between ACA/MCA territories
This pattern suggests global hypoperfusion rather than single-vessel occlusion.
Step 1 Study Strategy: From Memorization to Understanding
Building Anatomical Mental Models
Instead of memorizing isolated facts, build interconnected mental models:
1. Start with gross anatomy: Learn the physical locations of structures before studying their functions
2. Add functional correlations: Connect each anatomical structure to its physiological role
3. Layer on pathology: Understand how damage to each structure causes specific symptoms
4. Practice pattern recognition: Use question banks to reinforce anatomy-symptom relationships
The key is building these models systematically. When studying the basal ganglia, dont just memorize "Parkinson = bradykinesia." Understand the circuit: substantia nigra produces dopamine → dopamine facilitates the direct pathway → direct pathway promotes movement → loss of dopamine reduces movement facilitation → bradykinesia results.
Question Bank Strategy for Neurology
Neurology questions test pattern recognition more than pure memorization. Effective question practice involves:
First pass: Focus on identifying the anatomical location being tested. Dont worry about getting answers right initially. Second pass: Analyze why wrong answers are incorrect. Often they represent lesions in adjacent anatomical structures. Third pass: Time yourself and simulate exam conditions. By this point, you should recognize patterns quickly.
Practice with dedicated neurology question sets that focus on anatomy-symptom correlations rather than rare clinical scenarios.
Memory Techniques for High-Yield Lists
Certain neurology facts require precise memorization. Use these evidence-based techniques:
Cranial nerve functions: Create a story linking all 12 nerves in order. "Oh Oh Oh To Touch And Feel Very Good Velvet, Ah Heaven" for olfactory, optic, oculomotor, trochlear, trigeminal, abducens, facial, vestibulocochlear, glossopharyngeal, vagus, spinal accessory, hypoglossal. Spinal tract locations: Visualize the spinal cord cross-section as a clock. Dorsal columns at 12 oclock, corticospinal tracts at 6 oclock, spinothalamic tracts at 3 and 9 oclock. Basal ganglia connections: Use the "go/stop" framework. Direct pathway = go signal, indirect pathway = stop signal, dopamine tips the balance toward go.
Practice Integration: Putting It All Together
Sample Vignette Analysis
"A 45-year-old man presents with sudden onset of right-sided weakness affecting his face and arm more than his leg. He has difficulty speaking but appears to understand commands. On examination, he has a right facial droop, right arm drift, and hyperreflexia on the right side."
Step 1 - Localize: Right-sided weakness with face > arm > leg pattern suggests left MCA territory. Understanding of speech with impaired expression suggests Broca area involvement. Step 2 - Identify pathway: Left MCA supplies left motor cortex (causing right weakness) and Broca area in dominant hemisphere (causing non-fluent aphasia). Step 3 - Syndrome recognition: Left MCA stroke with Broca aphasia.
This systematic approach works for any neurology vignette on Step 1.
Common Step 1 Neurology Patterns
Recognize these high-yield question patterns:
Cranial nerve deficits → brainstem localization
Crossed sensory findings → spinothalamic vs dorsal column lesions
Movement disorders → basal ganglia pathway analysis
Language deficits → dominant hemisphere localization
Visual field cuts → optic pathway lesion localization
Gait abnormalities → cerebellum vs motor cortex vs spinal cord
Each pattern tests the same core skill: anatomical localization from symptom patterns.
Frequently Asked Questions
How much time should I spend on neuroanatomy vs neuropathology?
Spend 70% of your time on neuroanatomy and 30% on pathology. Step 1 neurology is fundamentally an anatomy exam disguised as clinical scenarios. Once you master the anatomical relationships, the pathology becomes logical consequences rather than random facts to memorize.
Which neurology topics are highest yield for Step 1?
Focus on these core areas in order: spinal cord tracts and syndromes, cranial nerve anatomy and pathways, basal ganglia circuitry, cerebral cortex localization, and brainstem organization. These five areas account for about 80% of Step 1 neurology questions.
How do I distinguish between similar neurological syndromes?
Build comparison charts highlighting the key distinguishing features. For example, Brown-Séquard has ipsilateral motor loss but contralateral sensory loss, while anterior cord syndrome has bilateral motor and sensory loss but preserved dorsal column function. The anatomical basis explains the clinical differences.
Should I memorize every rare neurological disease?
No. Step 1 tests common pathways and mechanisms, not rare zebra diagnoses. Focus on the major diseases that illustrate important pathophysiological principles: MS for demyelination, ALS for motor neuron degeneration, Huntington for basal ganglia dysfunction, Alzheimer for protein aggregation.
How can I improve my speed on neurology questions?
Practice anatomical localization drills until pattern recognition becomes automatic. When you see "loss of fine touch but preserved pain sensation," you should immediately think "dorsal column lesion" without consciously working through the anatomy. Speed comes from pattern recognition, not faster thinking.
What's the best way to review neurology before the exam?
Focus on high-yield anatomy diagrams and pathway flowcharts rather than rereading detailed text. Practice rapid-fire questions emphasizing localization skills. Review your incorrectly answered questions to identify knowledge gaps in specific anatomical areas.
---
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 1. Download free on Android and iOS.