Back
How to Study Neurology for USMLE Step 2 CK 2026: High-Yield Topics, Clinical Vignette Strategy and Exam Checklist
Master USMLE Step 2 CK neurology with this complete guide covering stroke management, seizure protocols, headache differentials, and clinical vignette strategies for exam success.
How to Study Neurology for USMLE Step 2 CK 2026: High-Yield Topics, Clinical Vignette Strategy and Exam Checklist
You are probably thinking: "Neurology was tough enough in med school, and now I have to master it for Step 2 CK?" Here is the truth — Step 2 CK neurology isnt about memorizing cranial nerve pathways or reciting anatomical tracts. Its about making the right management decision when faced with a 55-year-old with sudden aphasia or a 23-year-old with first-time seizure.
Step 2 CK tests your clinical reasoning through vignettes. The exam wants to know: can you identify the lesion location from the symptom cluster, determine urgency, and pick the next best step? When you see "thunderclap headache + neck stiffness," your brain should immediately think: subarachnoid hemorrhage → CT head → LP if CT negative → 4-vessel angiography. That reflex — from presentation to action sequence — is what separates high scorers from the rest.
This guide teaches you the exact framework that works: recognize the pattern, determine urgency, execute the algorithm. Every high-yield neurology topic is covered with the management sequences that actually appear on exam day.
The Step 2 CK Neurology Mindset: Management Over Memorization
Forget what you learned for Step 1. Step 2 CK neurology is about decisions, not diagrams. When you see a vignette, ask three questions:
1. What is the lesion location? (based on symptom cluster)
2. How urgent is this? (emergent vs urgent vs routine workup)
3. What is the next best step? (imaging, lab, treatment, or referral)
The exam loves testing management sequences where students commonly mess up the order. Give antibiotics before lumbar puncture? Wrong — unless there are signs of increased intracranial pressure. Start AED after first unprovoked seizure? Wrong — workup first, then observe. Give glucose before thiamine in altered mental status? Wrong — Wernicke encephalopathy can be precipitated.
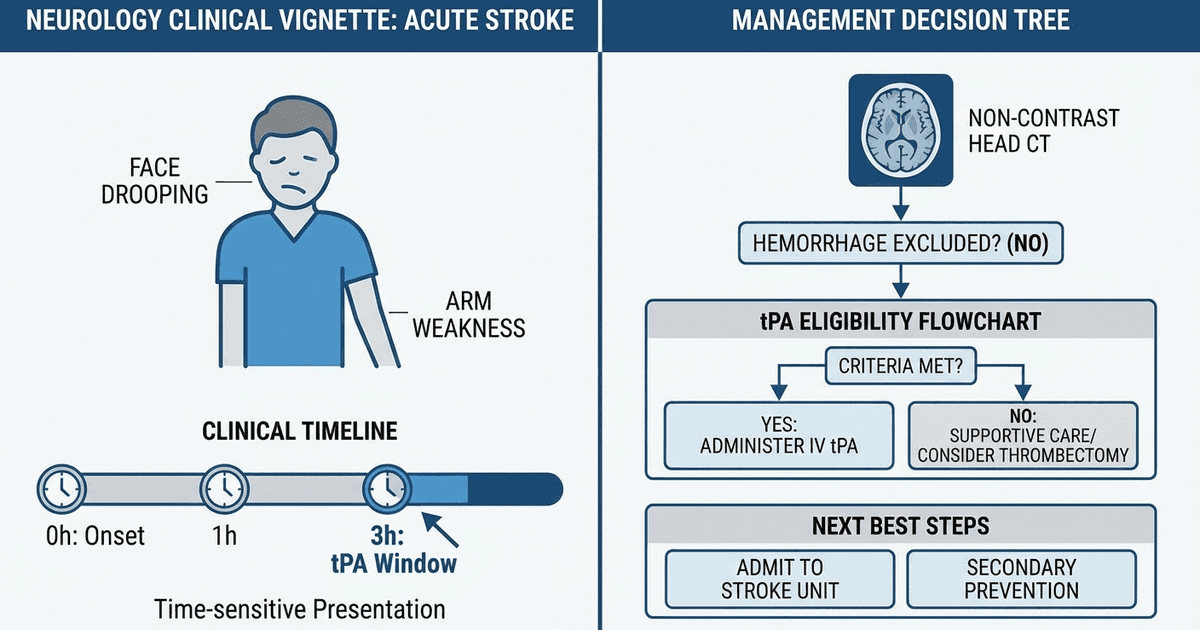
Clinical Rounds trains exactly this decision-tree thinking through scenario-based practice. When you encounter "55-year-old with sudden right arm weakness and aphasia — what is the next best step?" the platform builds your reflex: CT head first → exclude hemorrhage → check tPA eligibility → time window → administer or not. This is examiner logic for neurology vignettes.
High-Yield Stroke Management: Time Windows and Decision Points
Stroke questions are guaranteed on Step 2 CK. The key is knowing the time-sensitive algorithms.
Acute Ischemic Stroke Protocol
Presentation: Sudden focal neurological deficit (hemiparesis, aphasia, visual field cut) Management sequence: 1. CT head immediately (to exclude hemorrhage) 2. Check time of symptom onset 3. tPA eligibility window: 3-4.5 hours from onset 4. If eligible: Give tPA (alteplase) 0.9 mg/kg IV 5. If not eligible: Aspirin 325mg daily Key exam traps:
Never give tPA without CT head first
Recent surgery, active bleeding, or BP >185/110 are contraindications
NIHSS score helps determine severity but doesnt change acute management
Carotid ultrasound comes later — not in acute setting
Hemorrhagic Stroke Management
Presentation: Sudden severe headache + focal deficits, often with nausea/vomiting Management: 1. Stop all anticoagulants immediately 2. BP control: Target <140/90 (avoid aggressive reduction) 3. No tPA ever 4. Neurosurgery consult if large bleed or midline shift
TIA (Transient Ischemic Attack)
Definition: Neurological symptoms that resolve within 24 hours (usually <1 hour) Management: 1. Aspirin + dipyridamole OR clopidogrel 2. High-intensity statin (atorvastatin 80mg) 3. Carotid duplex ultrasound 4. If carotid stenosis >70%: Carotid endarterectomy within 2 weeks
When dealing with stroke management sequences, students often miss critical details about timing and contraindications. The status epilepticus management lessons cover similar emergency protocols where sequence matters.
Headache Presentations: Recognition and Red Flags
Headache questions test your ability to distinguish benign from life-threatening causes. Know the red flags and their workups.
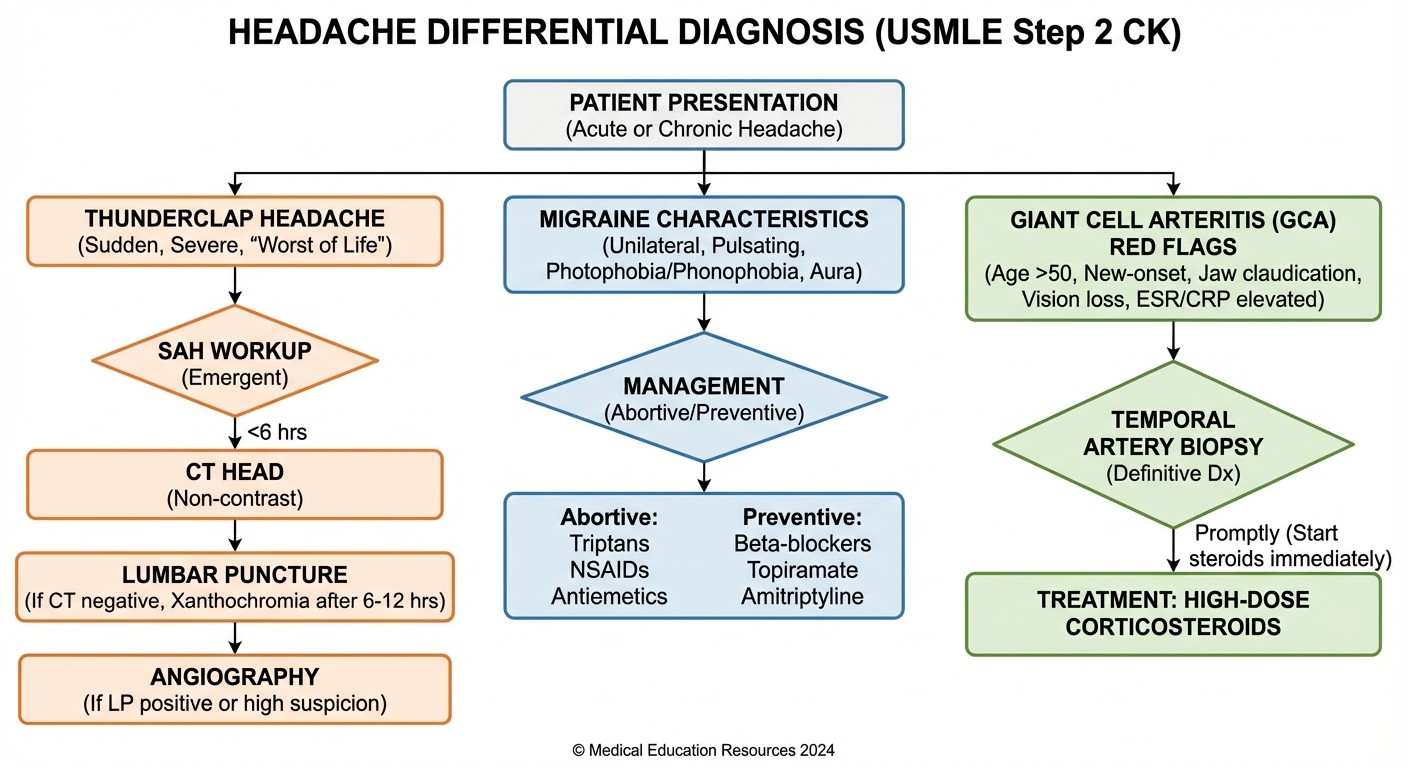
Subarachnoid Hemorrhage (SAH)
Classic presentation: "Worst headache of my life" — thunderclap onset, reaches maximum intensity in seconds Workup sequence: 1. CT head (95% sensitive if done within 12 hours) 2. If CT negative: Lumbar puncture looking for xanthochromia 3. If LP positive: 4-vessel cerebral angiography to find aneurysm Management: Neurosurgery consult, nimodipine to prevent vasospasm, blood pressure control
Giant Cell Arteritis (GCA)
Presentation: Age >50, temporal headache, jaw claudication, visual symptoms Red flag: Sudden unilateral vision loss = ophthalmologic emergency Workup: 1. ESR >50 (usually >100) 2. Temporal artery biopsy (gold standard) 3. Start prednisone immediately — dont wait for biopsy results Key point: Visual loss can be permanent if treatment is delayed
Primary Headache Patterns
Type | Pattern | Triggers | Treatment |
|---|---|---|---|
Migraine | Unilateral, throbbing, 4-72h | Stress, hormones, foods | Sumatriptan (acute), propranolol (prevention) |
Cluster | Unilateral periorbital, 15min-3h | Alcohol, sleep changes | 100% oxygen, sumatriptan |
Tension | Bilateral, pressing, hours-days | Stress, muscle tension | NSAIDs, stress management |
Explanation Chat immediately breaks down the reasoning when students miss headache vignettes: why this management step comes before that one, what the underlying pathophysiology mandates, and what the next best step truly is.
Seizure Management: When to Start AED and Emergency Protocols
Seizure questions focus on two scenarios: first unprovoked seizure (when NOT to start medication) and status epilepticus (emergency management sequence).
First Unprovoked Seizure
Management: Do NOT start AED after first seizure Workup: 1. EEG (to look for epileptiform activity) 2. Brain MRI (to exclude structural cause) 3. Basic labs: glucose, electrolytes, toxicology screen 4. Only start AED if: second seizure occurs Key exam trap: Students want to start medication immediately — resist this urge
Status Epilepticus Protocol
Definition: Seizure >5 minutes OR recurrent seizures without recovery Management sequence (memorize this order): 1. Lorazepam 4mg IV (first-line benzodiazepine) 2. If continues: Fosphenytoin 20mg/kg IV 3. If still continues: Phenobarbital 20mg/kg IV 4. If refractory: Propofol or midazolam drip
The status epilepticus flashcards use spaced repetition to drill these sequences until theyre automatic — exactly what you need when the exam throws time-sensitive emergency scenarios.
AED Selection by Seizure Type
Seizure Type | First-Line AED | Key Points |
|---|---|---|
Absence | Ethosuximide | Child staring spells, 3-Hz spike-wave |
Focal | Carbamazepine | Most common adult seizure type |
Generalized tonic-clonic | Phenytoin or carbamazepine | Avoid in absence seizures |
Myoclonic | Valproic acid | Avoid carbamazepine (can worsen) |
Altered Mental Status: AEIOU TIPS Framework
Altered mental status vignettes test systematic approach to delirium, dementia, and metabolic causes.
AEIOU TIPS Mnemonic
A: Alcohol, Acidosis
E: Encephalopathy (hepatic, uremic), Electrolytes, Endocrine
I: Insulin (hypo/hyperglycemia), Infection
O: Opiates, Oxygen (hypoxia)
U: Uremia
T: Trauma, Temperature (hypo/hyperthermia), Toxins
I: Infection
P: Psychiatric, Poisoning
S: Seizure, Stroke, Syncope
Wernicke Encephalopathy
Classic triad: Confusion, ataxia, ophthalmoplegia Critical management rule: Always give thiamine BEFORE glucose Why: Glucose can precipitate Wernicke in thiamine-deficient patients Treatment: Thiamine 100mg IV, then glucose
Delirium vs Dementia vs Depression
Feature | Delirium | Dementia | Depression |
|---|---|---|---|
Onset | Acute (hours-days) | Gradual (months-years) | Weeks-months |
Consciousness | Fluctuating | Normal | Normal |
Attention | Impaired | Normal early | May be impaired |
Reversibility | Often reversible | Progressive | Treatable |
When working through altered mental status cases, Clinical Rounds helps build the systematic approach: "72-year-old with acute confusion — what is the next best step?" You learn to think: check vitals → glucose → electrolytes → infection workup → consider toxins.
Dementia Differentials: Clinical Patterns and Management
Step 2 CK tests dementia recognition and appropriate management, not just diagnosis.
Alzheimer Disease
Features: Gradual onset, memory loss first, preserved motor function Diagnosis: Clinical + neuropsychological testing, MRI to exclude other causes Treatment: Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) Advanced disease: Add memantine (NMDA receptor antagonist)
Lewy Body Dementia
Classic triad: Fluctuating cognition, visual hallucinations, parkinsonism Key management: Avoid antipsychotics (can cause severe reactions) Treatment: Cholinesterase inhibitors help cognitive symptoms
Vascular Dementia
Pattern: Stepwise cognitive decline, often after strokes Risk factors: Hypertension, diabetes, atherosclerosis Prevention: Control vascular risk factors
Normal Pressure Hydrocephalus
Triad: Gait instability ("magnetic gait"), urinary incontinence, dementia Imaging: Enlarged ventricles out of proportion to sulci Treatment: Ventriculoperitoneal shunt
Movement Disorders: Classic Presentations
Parkinson Disease
Clinical triad: Resting tremor, rigidity, bradykinesia Additional features: Masked facies, shuffling gait, micrographia Treatment:
Early disease: Dopamine agonists (pramipexole, ropinirole)
Advanced disease: Levodopa/carbidopa
Severe: Deep brain stimulation
Essential Tremor
Features: Bilateral action tremor, improves with alcohol Treatment: Propranolol (first-line) or primidone Key difference from Parkinson: No rigidity or bradykinesia
Huntington Disease
Genetics: Autosomal dominant, chromosome 4 Features: Choreiform movements, psychiatric symptoms, dementia Imaging: Caudate atrophy on MRI Management: Supportive care, genetic counseling
High-yield movement disorder facts are perfect for Synapses flashcards — the AI's spaced repetition engine surfaces cards like "Essential tremor vs Parkinson tremor characteristics" at exactly the right review intervals.
Peripheral Neuropathy and Cranial Nerve Disorders
Guillain-Barré Syndrome
Presentation: Ascending weakness starting in legs, areflexia CSF findings: Albuminocytologic dissociation (elevated protein >45, normal cell count <10) Treatment: IVIG or plasmapheresis (equally effective) Respiratory monitoring: Vital capacity, negative inspiratory force
Bell Palsy (CN VII)
Features: Unilateral facial weakness (forehead involved = LMN lesion) Treatment: Prednisone within 72 hours of onset Prognosis: 80% recover completely
Carpal Tunnel Syndrome
Signs: Thenar muscle wasting, positive Tinel and Phalen signs Confirmation: Nerve conduction studies + EMG Treatment: Wrist splinting, steroid injection, surgical release
Meningitis: Bacterial vs Viral Recognition
Bacterial Meningitis
CSF findings: Low glucose, high protein, neutrophilic pleocytosis Empiric treatment: Ceftriaxone + vancomycin + dexamethasone Critical rule: Give dexamethasone BEFORE or WITH first antibiotic dose Lumbar puncture timing: Do LP before antibiotics unless papilledema present
Viral Meningitis
CSF findings: Normal glucose, mild protein elevation, lymphocytic pleocytosis Treatment: Supportive care Exception: HSV encephalitis → acyclovir immediately
High-Yield Meningitis Vignettes
Meningococcemia: Headache + fever + petechial rash → give antibiotics before LP HIV patient with ring-enhancing lesion: Toxoplasmosis → empiric treatment for 2 weeks before biopsy College student with fever + headache: Think meningococcal → isolate + treat contacts
Clinical Vignette Strategy: Pattern Recognition
Step 2 CK neurology vignettes follow predictable patterns. Train your pattern recognition:
Stroke Patterns
Middle cerebral artery: Contralateral hemiparesis + aphasia (if dominant hemisphere)
Posterior cerebral artery: Contralateral homonymous hemianopia
Vertebrobasilar: Diplopia, vertigo, ataxia, cranial nerve deficits
Headache Red Flags
Thunderclap: SAH until proven otherwise
Age >50 + temporal headache: GCA workup
Fever + headache + rash: Meningococcal disease
Seizure Contexts
First seizure: Workup but dont start AED
HIV + ring-enhancing lesion: Toxoplasmosis
Alcohol withdrawal: Seizure risk peaks at 24-48 hours
The pattern recognition becomes automatic with practice. When students miss neurology MCQs, Explanation Chat converts "I guessed wrong" into durable management memory by breaking down the exact clinical reasoning.
High-Yield Exam Checklist
Stroke Management
[ ] CT head before tPA (always)
[ ] tPA window: 3-4.5 hours from onset
[ ] Aspirin if tPA not given
[ ] Carotid endarterectomy if stenosis >70%
Headache Red Flags
[ ] Thunderclap → SAH workup (CT → LP → angiography)
[ ] Age >50 + temporal → GCA (ESR, steroids immediately)
[ ] Xanthochromia = SAH even if CT negative
Seizure Protocols
[ ] First seizure: EEG + MRI, no AED
[ ] Status epilepticus: lorazepam → fosphenytoin → phenobarbital
[ ] AED by type: absence (ethosuximide), focal (carbamazepine)
Emergency Sequences
[ ] Thiamine BEFORE glucose (Wernicke prevention)
[ ] Antibiotics before LP (only if papilledema)
[ ] Dexamethasone WITH first antibiotic dose
Dementia Features
[ ] Alzheimer: gradual, memory first
[ ] Lewy body: fluctuating + hallucinations + parkinsonism
[ ] Vascular: stepwise decline
Practice these algorithms until theyre reflexive. Step 2 CK neurology rewards systematic thinking over memorization.
Frequently Asked Questions
How much neurology is on Step 2 CK?
Neurology comprises about 8-12% of Step 2 CK questions, typically 20-30 questions out of 280. Focus on high-yield topics like stroke, seizures, headaches, and movement disorders rather than trying to cover every neurological condition.
Do I need to memorize anatomical pathways for Step 2 CK neurology?
No. Step 2 CK focuses on clinical management, not anatomical details. Know functional anatomy (what happens when specific areas are damaged) but dont memorize detailed pathways. Focus on presentation patterns and management algorithms.
What's the most high-yield neurology topic for Step 2 CK?
Stroke management is the highest yield — it appears frequently and tests time-sensitive decision making. Master the tPA eligibility criteria, contraindications, and post-stroke management. Seizure protocols (especially status epilepticus) are second most important.
Should I start AED after a first unprovoked seizure?
No. The standard approach is workup (EEG + MRI) but observation without AED after the first seizure. Start AED only after a second seizure or if imaging shows a structural abnormality that increases recurrence risk.
How do I differentiate bacterial from viral meningitis?
CSF analysis is key: bacterial shows low glucose (<40), high protein (>100), and neutrophilic pleocytosis. Viral shows normal/mild low glucose, mild protein elevation, and lymphocytic pleocytosis. Clinical context matters — bacterial presents more acutely with higher fever.
What's the biggest mistake students make on neurology vignettes?
Rushing to treatment without proper workup sequence. Common errors: giving tPA without CT head first, starting AED after first seizure, giving glucose before thiamine, or doing LP in the presence of papilledema. Always follow the established protocols step by step.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE Step 2 CK. Download free on Android and iOS.