Back
NEET PG Renal Pharmacology Glossary 2026: Diuretics, ACE Inhibitors, ARBs and Calcineurin Inhibitors
Complete high-yield renal pharmacology reference for NEET PG 2026. Master diuretics, ACE inhibitors, ARBs, calcineurin inhibitors with mechanisms, side effects, and MCQ mnemonics.
NEET PG Renal Pharmacology Glossary 2026: Diuretics, ACE Inhibitors, ARBs and Calcineurin Inhibitors
You're probably staring at a renal pharmacology question right now, trying to remember whether furosemide causes hypokalemia or hyperkalemia. NEET PG loves testing renal drugs — they show up in 12-15 questions every year across nephrology, medicine, and pharmacology sections. The examiners know these drug mechanisms separate serious candidates from surface-level memorizers.
This glossary covers the 4 highest-yield renal drug classes: diuretics (all 5 types), ACE inhibitors, ARBs, and calcineurin inhibitors. Each entry includes mechanism, key drugs, side effects, contraindications, and battle-tested mnemonics that actually stick under exam pressure.
Skip the textbook chapters. This is your rapid-fire reference for the renal pharmacology that matters in NEET PG 2026.
Diuretics: Complete Drug Class Breakdown
Diuretics are the workhorses of renal pharmacology. NEET PG tests their mechanisms, side effect patterns, and clinical applications relentlessly. Master these 5 categories and you've secured 6-8 questions.
Loop Diuretics (High-Ceiling Diuretics)
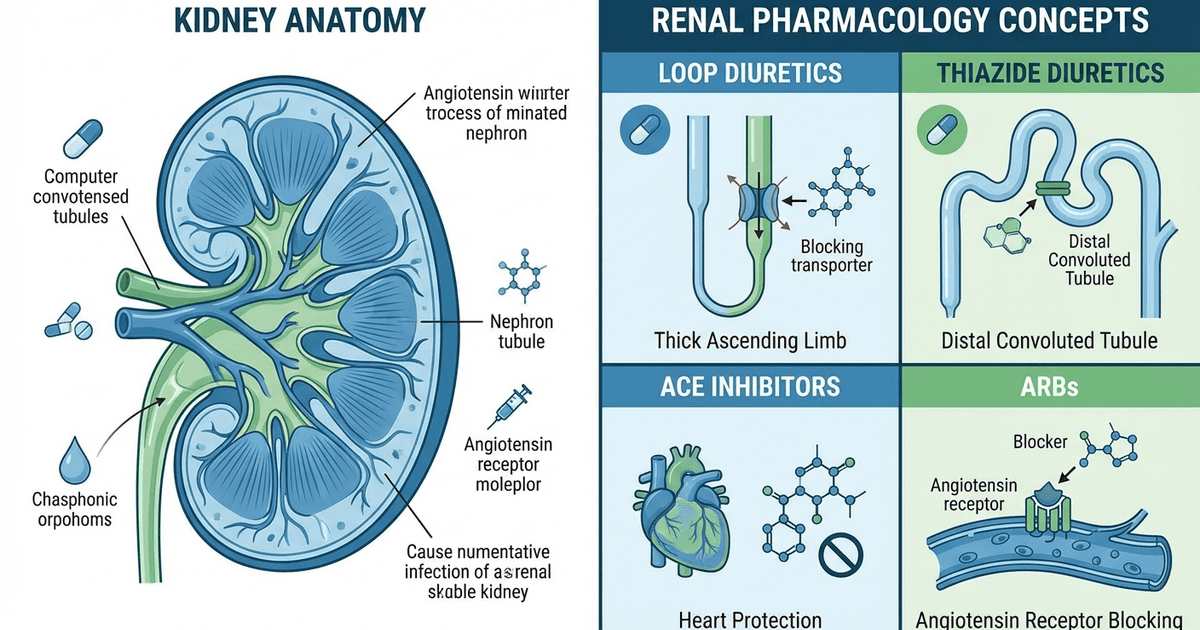
Key Drugs: Furosemide, Bumetanide, Torsemide, Ethacrynic acid Mechanism: Block Na-K-2Cl cotransporter (NKCC2) in thick ascending limb of loop of Henle. Prevents 25% of filtered sodium reabsorption — the most potent diuretic effect. Pharmacokinetics:
Onset: IV (5 mins), PO (30-60 mins)
Duration: 6-8 hours
Protein bound (95-99%)
Renal elimination
Clinical Uses:
Acute pulmonary edema (first-line)
Heart failure with fluid overload
Nephrotic syndrome
Acute renal failure (non-oliguric)
Side Effects (High-Yield for MCQs):
Hypokalemia (most tested)
Hyponatremia, hypomagnesemia
Hyperuricemia
Ototoxicity (especially ethacrynic acid)
Nephrotoxicity
Glucose intolerance
Mnemonic - Loop Side Effects: "LOOPS KILL"
Loss of potassium (hypokalemia)
Ototoxicity
Oliguria (nephrotoxicity)
PH imbalance (metabolic alkalosis)
Sugar high (hyperglycemia)
Kidney stones (hyperuricemia)
Infection risk
Loss of hearing
Loss of sodium/magnesium
When studying loop diuretics on Oncourse's adaptive flashcards, the spaced-repetition system surfaces side-effect cards right before they fade from memory — so you retain "furosemide → hypokalemia" without brute-force cramming.
Thiazide and Thiazide-Like Diuretics
Key Drugs: Hydrochlorothiazide (HCTZ), Chlorthalidone, Indapamide Mechanism: Block Na-Cl cotransporter (NCCT) in distal convoluted tubule. Prevents 10% of filtered sodium reabsorption. Pharmacokinetics:
Onset: 2-4 hours
Duration: 12-24 hours (chlorthalidone: 48-72 hours)
Renal elimination
Clinical Uses:
Hypertension (first-line)
Heart failure (mild)
Nephrogenic diabetes insipidus
Hypercalciuria/kidney stones
Side Effects:
Hypokalemia, hyponatremia
Hypercalcemia (opposite of loops)
Hyperuricemia
Glucose intolerance
Sexual dysfunction (males)
Mnemonic - Thiazide Effects: "THINK GLUCOSE UP"
Thirty percent glucose rise
Hypokalemia
Impotence
Na loss (hyponatremia)
Kidney stones prevented (hypercalciuria ↓)
Glucose up
Lipids up
Uric acid up
Calcium up
Osteoporosis prevented
Sexual problems
Ears safe (no ototoxicity)
Urination decreased over time
Potassium down
Potassium-Sparing Diuretics
#### Aldosterone Receptor Antagonists
Key Drugs: Spironolactone, Eplerenone Mechanism: Block mineralocorticoid receptors in collecting duct. Prevent aldosterone-mediated Na reabsorption and K secretion. Clinical Uses:
Heart failure (mortality benefit with ACE-I)
Primary hyperaldosteronism
Ascites (cirrhosis)
Hypertension
Side Effects:
Hyperkalemia (dangerous with ACE-I)
Gynecomastia (spironolactone only)
Sexual dysfunction
#### Epithelial Sodium Channel Blockers
Key Drugs: Amiloride, Triamterene Mechanism: Directly block epithelial sodium channels (ENaC) in collecting duct. Clinical Uses:
Lithium-induced nephrogenic DI
Combined with thiazides
Side Effects:
Hyperkalemia
Metabolic acidosis
Mnemonic - K-Sparing Diuretics: "SPARE THE K"
Spironolactone (gynecomastia)
Potassium retention
Amiloride (direct ENaC block)
Receptor antagonist (spironolactone)
Eplerenone (selective)
Triamterene
Hyperkalemia risk
ENaC blockade (amiloride/triamterene)
Carbonic Anhydrase Inhibitors
Key Drug: Acetazolamide Mechanism: Inhibits carbonic anhydrase in proximal tubule. Prevents Na-HCO3 reabsorption, causing bicarbonate loss. Clinical Uses:
Glaucoma (primary indication)
Altitude sickness
Epilepsy (adjunct)
Pseudotumor cerebri
Side Effects:
Metabolic acidosis (HCO3 loss)
Hypokalemia
Kidney stones (calcium phosphate)
Paresthesias
Practice carbonic anhydrase inhibitor mechanisms with targeted renal pharmacology MCQs — each question comes with detailed AI explanations that map the physiology → drug mechanism → side effect chain.
Osmotic Diuretics
Key Drug: Mannitol Mechanism: Creates osmotic gradient in tubular fluid. Prevents water reabsorption throughout nephron. Clinical Uses:
Cerebral edema
Acute glaucoma
Acute renal failure (prevention)
Drug overdose (enhance elimination)
Side Effects:
Volume expansion (initially)
Pulmonary edema
Electrolyte imbalance
Acute renal failure (paradoxically)
Contraindications:
Anuria
Severe heart failure
Pulmonary edema
ACE Inhibitors: Mechanism and Clinical Pearls
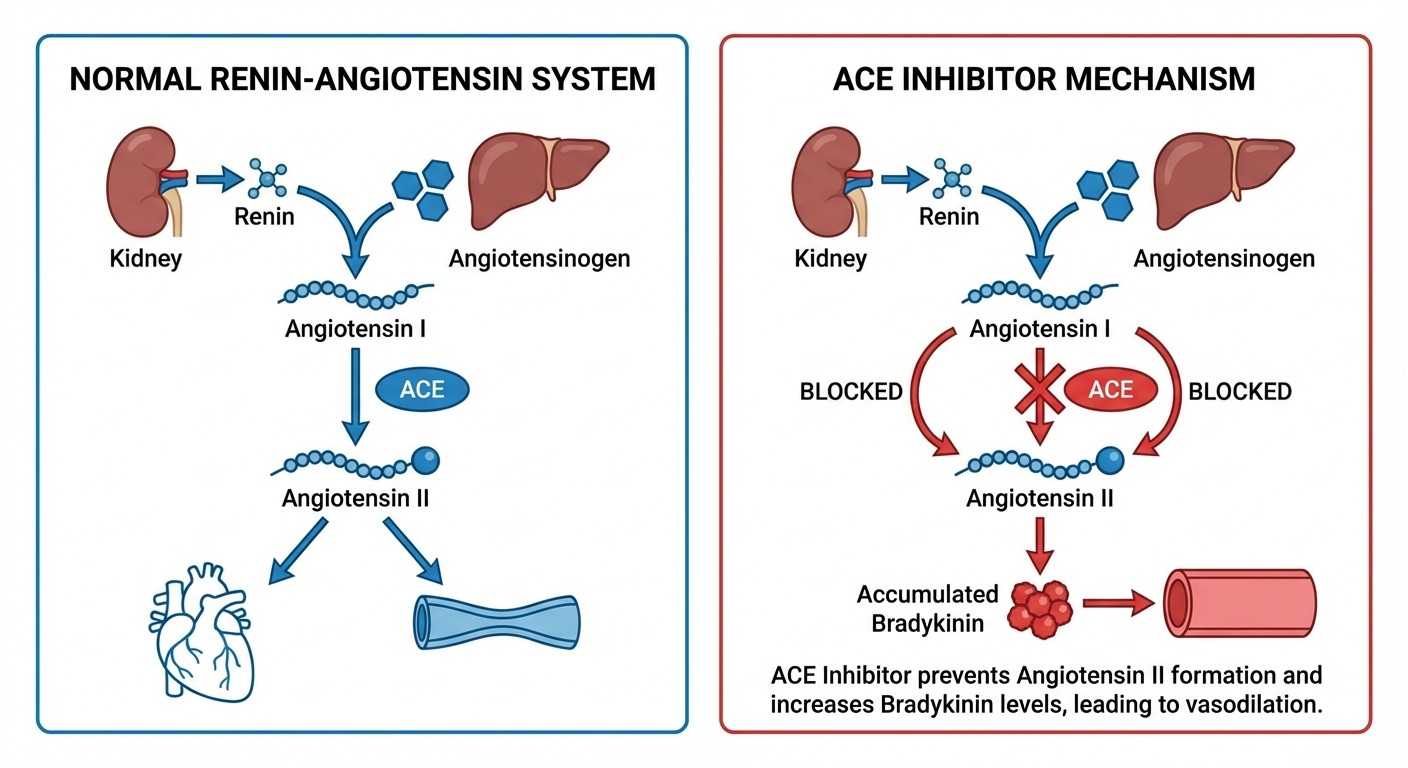
Key Drugs: Captopril, Enalapril, Lisinopril, Ramipril, Perindopril Mechanism: Block angiotensin-converting enzyme (ACE). Prevents conversion of angiotensin I to angiotensin II. Also prevents bradykinin degradation.
Pharmacokinetics:
Captopril: Short-acting (8 hours), needs TID dosing
Enalapril: Prodrug, needs conversion to enalaprilat
Lisinopril: Long-acting, no hepatic metabolism
Clinical Uses:
Hypertension (first-line)
Heart failure (mortality benefit)
Post-MI (within 24 hours)
Diabetic nephropathy
Proteinuria
Side Effects (NEET PG Favorites):
Dry cough (10-15% patients, due to bradykinin)
Hyperkalemia
Angioedema (rare but dangerous)
Acute renal failure (bilateral renal artery stenosis)
First-dose hypotension
Mnemonic - ACE Inhibitor Side Effects: "ACE COUGH"
Angioedema
Cough (dry, persistent)
Elevated potassium
Creatinine rise
Orthostatic hypotension
Uremia (in bilateral RAS)
GFR decrease
Hypotension (first dose)
Contraindications:
Bilateral renal artery stenosis
Pregnancy (teratogenic)
Hyperkalemia
Angioedema history
Master ACE inhibitor mechanisms through Oncourse's pharmacology lessons, then reinforce with targeted practice questions that test real NEET PG scenarios.
Angiotensin Receptor Blockers (ARBs): The Cough-Free Alternative
Key Drugs: Losartan, Valsartan, Telmisartan, Candesartan, Olmesartan Mechanism: Block angiotensin II type 1 (AT1) receptors. Prevent angiotensin II effects without affecting bradykinin metabolism. Pharmacokinetics:
Losartan: Active metabolite (E-3174)
Telmisartan: Longest half-life (24 hours)
Most are prodrugs requiring hepatic conversion
Clinical Uses:
Hypertension (especially with ACE-I intolerance)
Heart failure (if ACE-I not tolerated)
Diabetic nephropathy
Post-MI (alternative to ACE-I)
Side Effects:
Generally better tolerated than ACE inhibitors
No cough (doesn't affect bradykinin)
Hyperkalemia
Angioedema (rare)
Hypotension
Mnemonic - ARB vs ACE: "ARBs Are Really Better"
Angioedema (still possible but rare)
Renal protection
Bradykinin unaffected (no cough)
Angiotensin blocked
RAS inhibition
Equality in efficacy
Really
Easy tolerance
Alternative to ACE
Lower cough risk
Long-acting options
Yields same benefits
Better
Endured by patients
Tolerated well
Teratogenic (still avoid pregnancy)
Effective in diabetics
Renoprotective
Students who struggle with RAAS pharmacology can benefit from Oncourse's adaptive targeting — the platform tracks performance by subject tag and serves more ACE inhibitor vs ARB questions until the distinction clicks.
Calcineurin Inhibitors: Immunosuppression with Renal Impact
Key Drugs: Cyclosporine, Tacrolimus (FK506) Mechanism: Inhibit calcineurin phosphatase. Prevent T-cell activation by blocking IL-2 transcription. Also cause renal vasoconstriction. Pharmacokinetics:
High protein binding
Extensive hepatic metabolism (CYP3A4)
Therapeutic drug monitoring required
Drug interactions common
Clinical Uses:
Organ transplantation (kidney, liver, heart)
Severe psoriasis
Rheumatoid arthritis
Nephrotic syndrome (minimal change disease)
Side Effects (High-Yield for NEET PG):
Nephrotoxicity (acute and chronic)
Hypertension
Neurotoxicity (tremor, seizures)
Gum hyperplasia (cyclosporine)
Hirsutism (cyclosporine)
Glucose intolerance (tacrolimus > cyclosporine)
Mnemonic - Cyclosporine Side Effects: "CYCLO SPORES"
Chronic nephrotoxicity
Yearning for glucose (diabetes)
Convulsions (neurotoxicity)
Liver toxicity
Osteoporosis
Skin changes
Pressure up (hypertension)
Oral problems (gum hyperplasia)
Renal damage
Excess hair (hirsutism)
Susceptible to infections
Drug Interactions:
CYP3A4 inducers (decrease levels): rifampin, phenytoin
CYP3A4 inhibitors (increase levels): ketoconazole, erythromycin
Nephrotoxic drugs: aminoglycosides, NSAIDs
High-Yield Drug Comparison Tables
Diuretic Mechanism Summary
Drug Class | Site of Action | Na+ Block % | K+ Effect | Ca2+ Effect | Mg2+ Effect |
|---|---|---|---|---|---|
Loop | Thick ascending limb | 25% | ↓ | ↓ | ↓ |
Thiazide | Distal convoluted tubule | 10% | ↓ | ↑ | ↓ |
K-sparing | Collecting duct | 2% | ↑ | No change | No change |
Carbonic anhydrase | Proximal tubule | 5% | ↓ | ↓ | ↓ |
Osmotic | Entire nephron | Variable | ↓ | ↓ | ↓ |
ACE Inhibitors vs ARBs: Key Differences
Feature | ACE Inhibitors | ARBs |
|---|---|---|
Cough incidence | 10-15% | <1% |
Mechanism | Block ACE enzyme | Block AT1 receptors |
Bradykinin effect | ↑ (causes cough) | No effect |
Angioedema risk | Higher | Lower |
Renal protection | Proven | Proven |
Heart failure benefit | First-line | Second-line |
Cost | Lower | Higher |
Nephrotoxicity Risk Ranking
Risk Level | Drugs |
|---|---|
High | Cyclosporine, Tacrolimus, Aminoglycosides |
Moderate | Loop diuretics (high dose), NSAIDs |
Low | Thiazides, ACE inhibitors, ARBs |
Protective | ACE inhibitors, ARBs (in diabetes) |
Clinical Scenarios: NEET PG Question Patterns
Scenario 1: Heart Failure Management
Question Pattern: "65-year-old with heart failure, already on ACE inhibitor and beta-blocker. Which diuretic provides mortality benefit?" Answer: Spironolactone (aldosterone antagonist) Key: Only K-sparing diuretic with proven mortality benefit in heart failure
Scenario 2: Hypertensive with Cough
Question Pattern: "Patient develops dry cough on enalapril. Best alternative?" Answer: ARB (losartan/valsartan) Key: ARBs dont affect bradykinin, so no cough
Scenario 3: Transplant Patient with Rising Creatinine
Question Pattern: "Kidney transplant patient on tacrolimus, creatinine rising. Most likely cause?" Answer: Calcineurin inhibitor nephrotoxicity Key: Chronic nephrotoxicity is dose-dependent and progressive
Drug Interaction Alert Box
Dangerous Combinations to Remember: 1. ACE-I + K-sparing diuretic = Hyperkalemia risk 2. Loop diuretic + Aminoglycoside = Ototoxicity ↑ 3. Cyclosporine + NSAID = Acute renal failure 4. Thiazide + Lithium = Lithium toxicity 5. ARB + ACE-I = Dual RAAS blockade (hyperkalemia, hypotension)
Check out our cardiovascular pharmacology glossary for more drug interaction patterns, and explore the complete NEET PG pharmacology series covering antimicrobials, CNS drugs, and endocrine agents.
Memory Palace Technique for Renal Drugs
Build a mental hospital ward where each room represents a drug class:
Room 1 (Emergency): Loop diuretics — patients with acute pulmonary edema, loud beeping monitors (ototoxicity), low potassium alarms Room 2 (General Ward): Thiazides — calm hypertensive patients, calcium supplements on bedside tables, glucose meters everywhere Room 3 (ICU): ACE inhibitors — heart failure patients, persistent cough sounds, "No Pregnancy" signs Room 4 (Private Room): ARBs — quiet patients (no cough), same heart benefits, premium pricing Room 5 (Transplant Unit): Calcineurin inhibitors — immunosuppressed patients, kidney function charts, blood level monitoring
Walk through this ward during exam prep, and the spatial memory will trigger drug details automatically.
Common NEET PG Mistakes to Avoid
1. Confusing thiazide calcium effects — Thiazides increase calcium (opposite of loops)
2. Missing ACE-I teratogenicity — Contraindicated in pregnancy (fetal renal dysgenesis)
3. Forgetting aldosterone antagonist mortality benefit — Spironolactone reduces death in heart failure
4. Ignoring drug monitoring — Calcineurin inhibitors need therapeutic levels
5. Mixing up osmotic diuretic indications — Mannitol for cerebral edema, not routine diuresis
Frequently Asked Questions
Which diuretic is safest in pregnancy?
Methyldopa is the first-line antihypertensive in pregnancy. Loop diuretics can be used if essential, but thiazides are avoided due to potential fetal complications. ACE inhibitors and ARBs are absolutely contraindicated.
Can ACE inhibitors and ARBs be used together?
Dual RAAS blockade is generally avoided due to increased risk of hyperkalemia, hypotension, and acute kidney injury. The combination provides no additional cardiovascular benefit over monotherapy.
What's the mechanism behind ACE inhibitor cough?
ACE normally breaks down bradykinin. When ACE is blocked, bradykinin accumulates in lung tissue, causing persistent dry cough in 10-15% of patients. ARBs dont affect bradykinin metabolism.
How do you monitor calcineurin inhibitor therapy?
Regular monitoring includes: serum creatinine, blood pressure, therapeutic drug levels (cyclosporine trough 100-200 ng/mL, tacrolimus trough 5-15 ng/mL), complete blood count, liver function tests, and glucose levels.
Which diuretic combination is most effective for resistant hypertension?
Thiazide + ACE inhibitor + calcium channel blocker is the preferred triple combination. Adding spironolactone as fourth-line agent can help resistant cases, but requires potassium monitoring.
Why do loop diuretics cause ototoxicity?
The inner ear has similar Na-K-2Cl transporters as the thick ascending limb. High-dose loop diuretics (especially ethacrynic acid) can damage these transporters, causing hearing loss or tinnitus.
Master renal pharmacology with the systematic approach this glossary provides, then reinforce your knowledge through spaced repetition on Oncourse's adaptive platform. The combination of high-yield content and intelligent practice transforms memorization into understanding.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.