USMLE Step 3 New Format 2026: What Changed and How to Prepare
USMLE Step 3 format changed in 2026: 9 CCS cases instead of 13, updated interface, adjusted timing. Complete guide to new format changes and updated study strategy.
USMLE Step 3 New Format 2026: What Changed and How to Prepare
You are probably staring at outdated Step 3 prep guides that still mention 13 CCS cases and 3.5-hour testing blocks. The USMLE Step 3 format changed significantly in 2026. Most resources online havent caught up yet.
The National Board of Medical Examiners (NBME) reduced CCS cases from 13 to 9, updated the interface, and adjusted timing across both testing days. If youre using a study plan built for the old format, youre wasting time on the wrong priorities.
Here's exactly what changed, what stayed the same, and how to adjust your prep strategy to match the new Step 3 format.
What the Old Step 3 Format Looked Like (Pre-2026)
Before 2026, USMLE Step 3 was a 2-day exam with this structure:
Day 1 (Old Format):
7 blocks of 46 MCQs each (322 total questions)
60 minutes per block
45 minutes total break time
Testing time: 7.5 hours
Day 2 (Old Format):
4 blocks of 46 MCQs each (184 total questions)
13 Computer-based Case Simulations (CCS)
25 minutes per CCS case
Testing time: 8 hours
The old format heavily weighted CCS cases. Students spent months practicing case management because those 13 simulations could make or break their score.
USMLE Step 3 New Format 2026: What Actually Changed
The National Board of Medical Examiners implemented these specific changes to Step 3 in 2026:
CCS Case Reduction
Old format: 13 CCS cases (5.4 hours of testing time)
New format: 9 CCS cases (3.75 hours of testing time)
Impact: 31% fewer cases to complete
Updated Interface
Cleaner navigation between case steps
Improved diagnostic ordering system
Enhanced patient monitoring displays
Streamlined medication dosing interface
Adjusted Timing Structure
Day 1 (2026 Format):
7 blocks of 46 MCQs each (322 total questions)
60 minutes per block
45 minutes total break time
Testing time: 7.5 hours (unchanged)
Day 2 (2026 Format):
4 blocks of 46 MCQs each (184 total questions)
9 Computer-based Case Simulations (CCS)
25 minutes per CCS case
Testing time: 6.75 hours (reduced from 8 hours)
What Stayed the Same
Total MCQ count: 506 questions across both days
Scoring methodology and passing standards
Content blueprint percentages
Basic case simulation format (History → Physical → Diagnostics → Treatment)
The key insight: fewer CCS cases means each one carries more weight, but youll have less time pressure overall.
Day 1 vs Day 2: How to Approach Each Testing Day
Day 1 Strategy: MCQ Marathon Endurance
Day 1 is pure multiple-choice endurance — 322 questions across 7.5 hours. Your energy management matters more than speed.
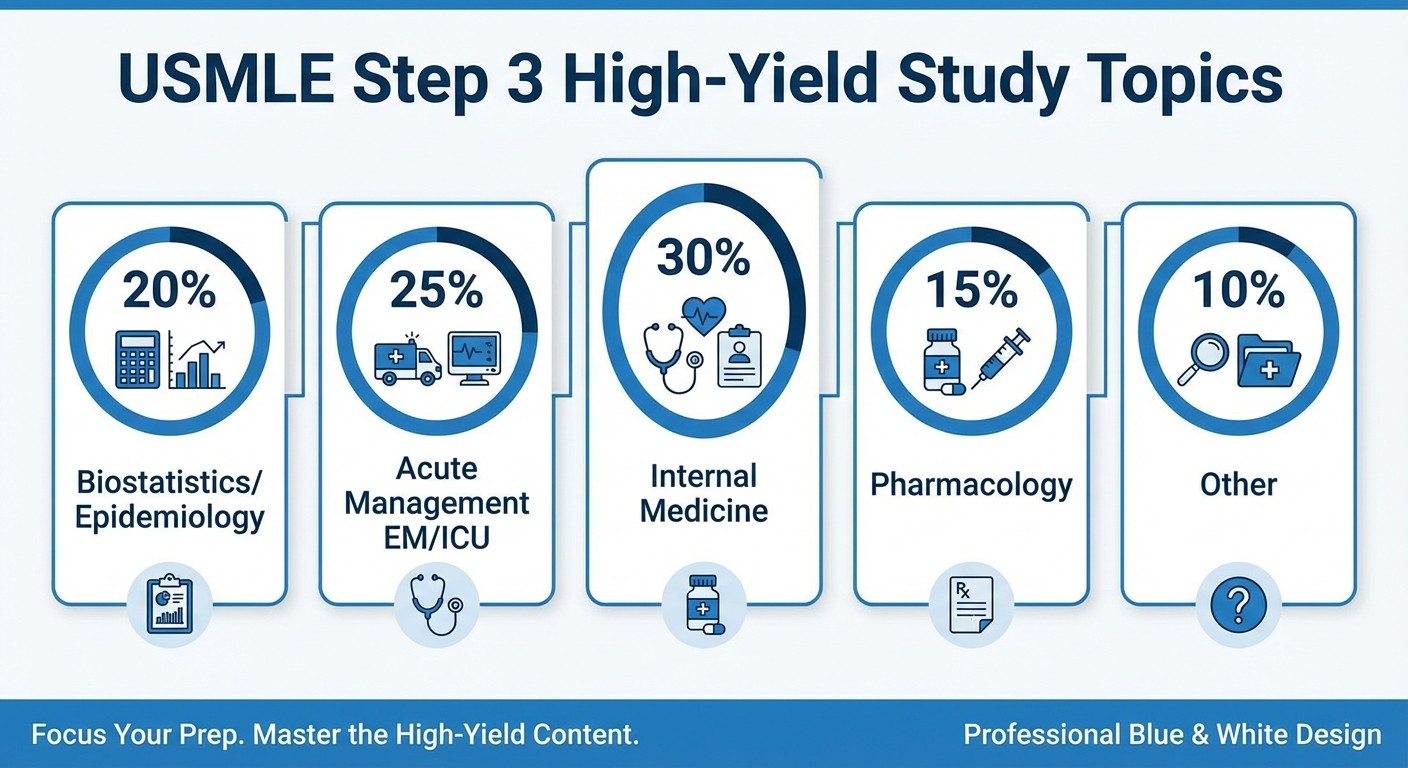
High-yield Day 1 topics:
Internal medicine (30% of questions)
Emergency medicine acute management
Pharmacology and drug interactions
Biostatistics and epidemiology
Preventive care and screening guidelines
Energy management tips:
Take a 5-minute break between every 2 blocks
Eat protein during longer breaks (not just snacks)
Dont second-guess answers after block 4 — decision fatigue sets in
After every wrong MCQ during practice, Rezzy auto-generates follow-up explanations with context-aware prompts. For Step 3's biostatistics blocks, this turns each mistake into a teaching moment about clinical reasoning chains.
Day 2 Strategy: MCQ + CCS Balance
Day 2 combines 4 MCQ blocks with 9 CCS cases. The format change means you need efficiency, not just thoroughness, in case simulations.
CCS case priorities (9 cases total):
Focus on common acute presentations (chest pain, dyspnea, altered mental status)
Master the interface before test day — know where to find vitals, labs, imaging
Practice efficient diagnostic ordering (avoid unnecessary tests that hurt your score)
MCQ vs CCS timing:
Complete MCQ blocks first (4 hours)
Use the 45-minute break to reset mentally for CCS
Tackle CCS cases in the final 3.75 hours
Oncourse's Clinical Rounds mirrors the exact CCS format — multi-step case simulation covering History Taking → Diagnostics → Differential → Treatment. The scoring engine penalizes unnecessary tests and rewards efficiency, matching how real Step 3 CCS cases are graded.
How to Adjust Your Study Timeline for the New Format
Months 1-2: Foundation Building
MCQ Focus (70% of study time):
Complete 2-3 full-length practice tests per week
Target high-yield internal medicine and emergency topics
Drill biostatistics calculations until theyre automatic
CCS Introduction (30% of study time):
Learn the interface and basic case flow
Practice 2-3 cases per week to build familiarity
Focus on common presentations, not rare diagnoses
Month 3: Integration and Practice
Balanced Approach (50/50 MCQ and CCS):
Simulate full Day 2 format: 4 MCQ blocks followed by 9 CCS cases
Time yourself strictly — 25 minutes per CCS case, no exceptions
Review every case for efficiency improvements
Common timing mistake: Students still allocate study time as if there were 13 CCS cases. With only 9 cases, spend more time on MCQ content review and less on case simulation volume.
Final 2 Weeks: Test-Taking Strategy
Take 2 full practice exams per week
Simulate exact testing conditions (7.5 hours Day 1, 6.75 hours Day 2)
Practice the new CCS interface until navigation feels automatic
The Daily Plan uses a 3-priority system for USMLE: next incomplete topic, lowest-accuracy revision (<60%), and spaced repetition for oldest material. Students dont need to manually juggle what to study each day.
High-Yield Study Strategy: Focus Areas That Matter
Biostatistics and Epidemiology (High-Yield)
Step 3 tests practical application of stats concepts, not just memorization. Focus on:
Essential calculations:
Number needed to treat (NNT) and number needed to harm (NNH)
Sensitivity, specificity, PPV, NPV in clinical scenarios
Relative risk, odds ratio interpretation
Confidence intervals and their clinical meaning
Study approach: Practice 10-15 biostat MCQs daily. Master the formulas first, then work through clinical applications. Questions often embed stats concepts within case presentations.
Work through biostatistics lessons and practice with biostatistics MCQs to solidify these concepts.
Acute Management (Emergency Medicine and ICU)
Both MCQs and CCS cases heavily test acute decision-making:
High-yield acute scenarios:
Chest pain workup (ACS vs PE vs aortic dissection)
Dyspnea evaluation (CHF vs pneumonia vs COPD exacerbation)
Altered mental status (hypoglycemia vs stroke vs sepsis)
Shock management (cardiogenic vs septic vs hypovolemic)
CCS case strategy: Start with vitals and basic labs. Order targeted diagnostics based on clinical suspicion. Avoid shotgun approaches — unnecessary tests hurt your score.
Practice case management through live simulations where you can build decision speed before the real exam.
Internal Medicine (Bread and Butter)
Internal medicine comprises 30% of Step 3 content. Focus on:
Chronic disease management:
Diabetes complications and monitoring
Hypertension treatment algorithms
Lipid management guidelines
COPD and asthma protocols
Pharmacology integration: Know drug interactions, contraindications, and monitoring requirements. Step 3 tests real-world prescribing decisions, not just mechanisms. Prevention and screening: Mammography schedules, colonoscopy guidelines, vaccination recommendations by age group.
Pharmacology and Drug Interactions
Step 3 pharmacology goes beyond basic mechanisms:
Focus areas:
Drug-drug interactions in polypharmacy patients
Dose adjustments for renal/hepatic impairment
Contraindications in pregnancy and elderly patients
Monitoring requirements for high-risk medications
Study tip: Create drug interaction cards for commonly tested combinations (warfarin + antibiotics, statins + fibrates, ACE inhibitors + NSAIDs).
Review pharmacology flashcards for spaced repetition of key drug concepts.
Common Mistakes to Avoid in the New Step 3 Format
Mistake 1: Over-Preparing CCS Cases
With 31% fewer CCS cases, students shouldnt spend 50% of their time on case simulations. The new format demands stronger MCQ performance.
Fix: Allocate 70% of study time to MCQs and 30% to CCS practice. Only increase CCS time if youre scoring below 60% on case simulations.
Mistake 2: Ignoring the New Interface
The updated CCS interface changes how you navigate cases. Students practicing on old simulators waste time relearning on test day.
Fix: Use practice platforms that match the 2026 interface. Spend 2-3 hours learning the new navigation before taking practice tests.
Mistake 3: Rushing Through Biostatistics
Many students guess on biostat questions to save time for "clinical" content. This backfires because biostat questions have clear right answers.
Fix: Master biostat calculations first. These questions take 30-45 seconds once you know the formulas, but 3-4 minutes if youre figuring them out during the exam.
Mistake 4: Memorizing CCS "Checklists"
Old prep strategies focused on memorizing order sets for each case type. The new format rewards clinical reasoning over rote memorization.
Fix: Practice case simulations that give feedback on efficiency and clinical decision-making. Understand why certain orders are appropriate, not just what to order.
Mistake 5: Studying Like Its Step 2 CK
Step 3 tests management decisions, not just diagnosis. Students often know the right diagnosis but choose suboptimal treatments.
Fix: For every condition you study, focus equally on diagnostic criteria AND management algorithms. Practice "next best step" thinking.
Practice Resources and Timeline Recommendations
Months 1-2: Foundation
MCQ volume: 150-200 questions per day
CCS practice: 3-4 cases per week
Focus: Content review with immediate question reinforcement
Goal: 65%+ accuracy on practice MCQs
Month 3: Integration
MCQ volume: 200-250 questions per day
CCS practice: 1 full 9-case simulation per week
Focus: Timed practice under exam conditions
Goal: 70%+ accuracy on practice MCQs, efficient CCS completion
Final 2 Weeks: Peak Performance
Practice tests: 2 full-length exams per week
CCS maintenance: 2-3 cases every other day
Focus: Test-taking strategy and endurance
Goal: Maintain performance under fatigue
Review comprehensive USMLE Step 3 study materials for detailed preparation strategies.
Frequently Asked Questions
How many CCS cases are on Step 3 in 2026?
Step 3 now includes 9 CCS cases instead of the previous 13. Each case still has a 25-minute time limit, but total CCS testing time decreased from 5.4 hours to 3.75 hours.
Did the Step 3 passing score change with the new format?
No, the passing score methodology remains the same. NBME adjusted scoring algorithms to account for fewer CCS cases, but the overall difficulty level is equivalent to previous years.
Should I spend more time on MCQs or CCS cases?
Focus 70% of study time on MCQs and 30% on CCS practice. With fewer cases, each CCS carries more weight, but MCQs still represent the majority of your score.
What's the biggest difference between old and new CCS interface?
The 2026 interface streamlines diagnostic ordering and patient monitoring displays. Navigation between case steps is cleaner, but the basic format (History → Physical → Diagnostics → Treatment) remains the same.
How long should I study for Step 3 with the new format?
Most students need 3-4 months of dedicated preparation. The reduced CCS volume doesnt significantly shorten study time because MCQ content review still requires the same depth.
Are there new topics tested in Step 3 2026?
Content blueprints remain unchanged. The format adjustments affect timing and interface, not the medical knowledge being tested.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for USMLE. Download free on Android and iOS.