NEET PG CNS Pharmacology Glossary 2026: Antidepressants, Antipsychotics, Antiepileptics and Opioids — High-Yield Drug Classes, Mechanisms and MCQ Mnemonics
Master CNS pharmacology for NEET PG 2026 with this comprehensive glossary covering antidepressants, antipsychotics, antiepileptics, and opioids. Includes mechanisms, mnemonics, and high-yield MCQ patterns.
NEET PG CNS Pharmacology Glossary 2026: Antidepressants, Antipsychotics, Antiepileptics and Opioids — High-Yield Drug Classes, Mechanisms and MCQ Mnemonics
CNS pharmacology accounts for roughly 18-22% of NEET PG pharmacology questions. Thats about 12-15 questions from just four drug classes. Most students waste time memorizing endless drug lists without understanding the core mechanisms. Here's the reality: NEET PG doesnt ask you to recite 50 antidepressants — it tests whether you can connect mechanism to side effect to clinical use in 63 seconds per question.
This glossary cuts through the noise. You'll get the high-yield drugs, their mechanisms, memorable mnemonics, and the exact MCQ patterns NEET PG repeats year after year. Every drug mentioned here has appeared in the last 5 years of NEET PG. Every mnemonic has been tested with students who scored 600+ ranks.
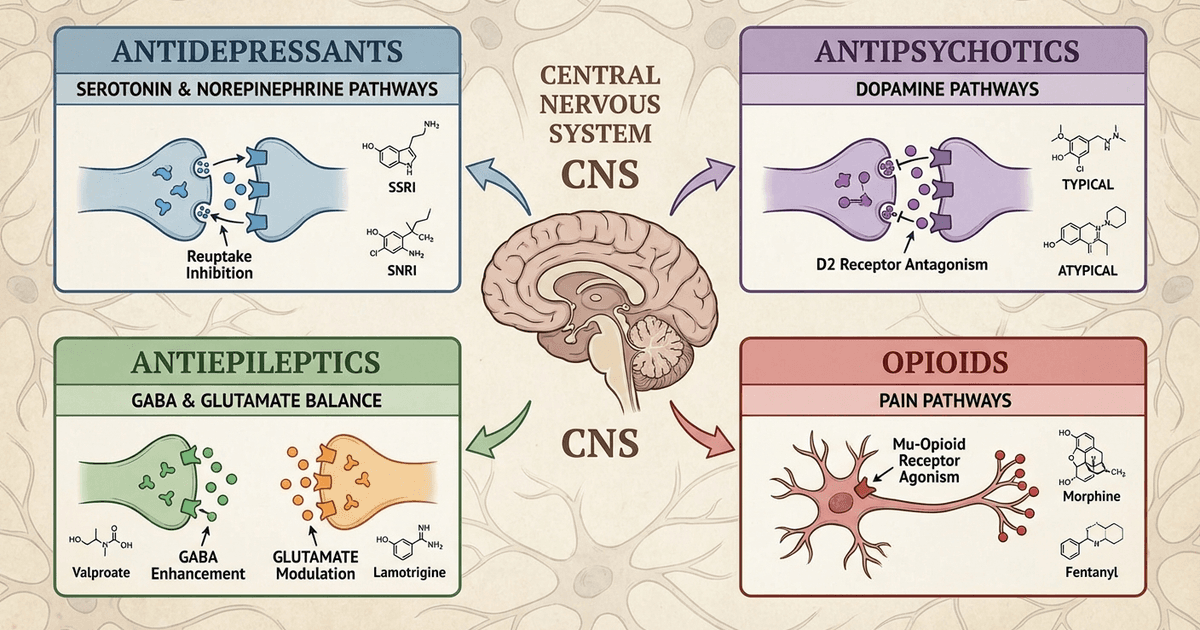
Antidepressants: The Monoamine Highway
SSRIs (Selective Serotonin Reuptake Inhibitors)
High-Yield Drugs: Fluoxetine, Sertraline, Escitalopram, Paroxetine Mechanism: Block serotonin transporter (SERT), increasing synaptic serotonin availability Mnemonic for SSRI side effects: "SSRI = Sexual Side-effects, Sleep problems, Serotonin syndrome, Rash"
Sexual dysfunction (most common)
Sleep disturbances
Serotonin syndrome risk
Rash/skin reactions
MCQ Pattern: NEET PG loves testing fluoxetine's longest half-life (2-4 days) vs other SSRIs (1 day). Also expect questions on serotonin syndrome triad: altered mental status, neuromuscular hyperactivity, autonomic instability.
For deeper understanding of SSRI mechanisms and clinical pharmacology, explore our NEET PG antidepressants lessons.
SNRIs (Serotonin-Norepinephrine Reuptake Inhibitors)
High-Yield Drugs: Venlafaxine, Duloxetine Mechanism: Dual reuptake inhibition of serotonin and norepinephrine Mnemonic for SNRI advantages: "SNRI = Superior for Neuropathy, Robust for Insomnia"
Better for neuropathic pain (duloxetine)
Effective for depression with somatic symptoms
Clinical Pearl: Duloxetine is the only antidepressant specifically indicated for diabetic neuropathy. NEET PG frequently tests this unique indication.
Tricyclic Antidepressants (TCAs)
High-Yield Drugs: Imipramine, Amitriptyline, Nortriptyline Mechanism: Block reuptake of serotonin and norepinephrine, plus anticholinergic and antihistaminic effects Mnemonic for TCA side effects: "TCA = Terrible Cardiotoxicity Always"
QT prolongation and arrhythmias
Anticholinergic effects (dry mouth, constipation, urinary retention)
Sedation and weight gain
MCQ Trap: Remember imipramine is first-line for nocturnal enuresis in children, not depression. Practice with TCA pharmacology questions to master these distinctions.
Atypical Antidepressants
Bupropion: Dopamine and norepinephrine reuptake inhibitor
Unique feature: No sexual side effects, may increase libido
Contraindication: Seizure disorders
Mnemonic: "Bupropion = Better Performance (sexual), Bad for seizures"
Mirtazapine: Alpha-2 antagonist, antihistaminic
Unique feature: Causes weight gain and sedation
Clinical use: Depression with insomnia and poor appetite
Antipsychotics: Dopamine's Double-Edged Sword
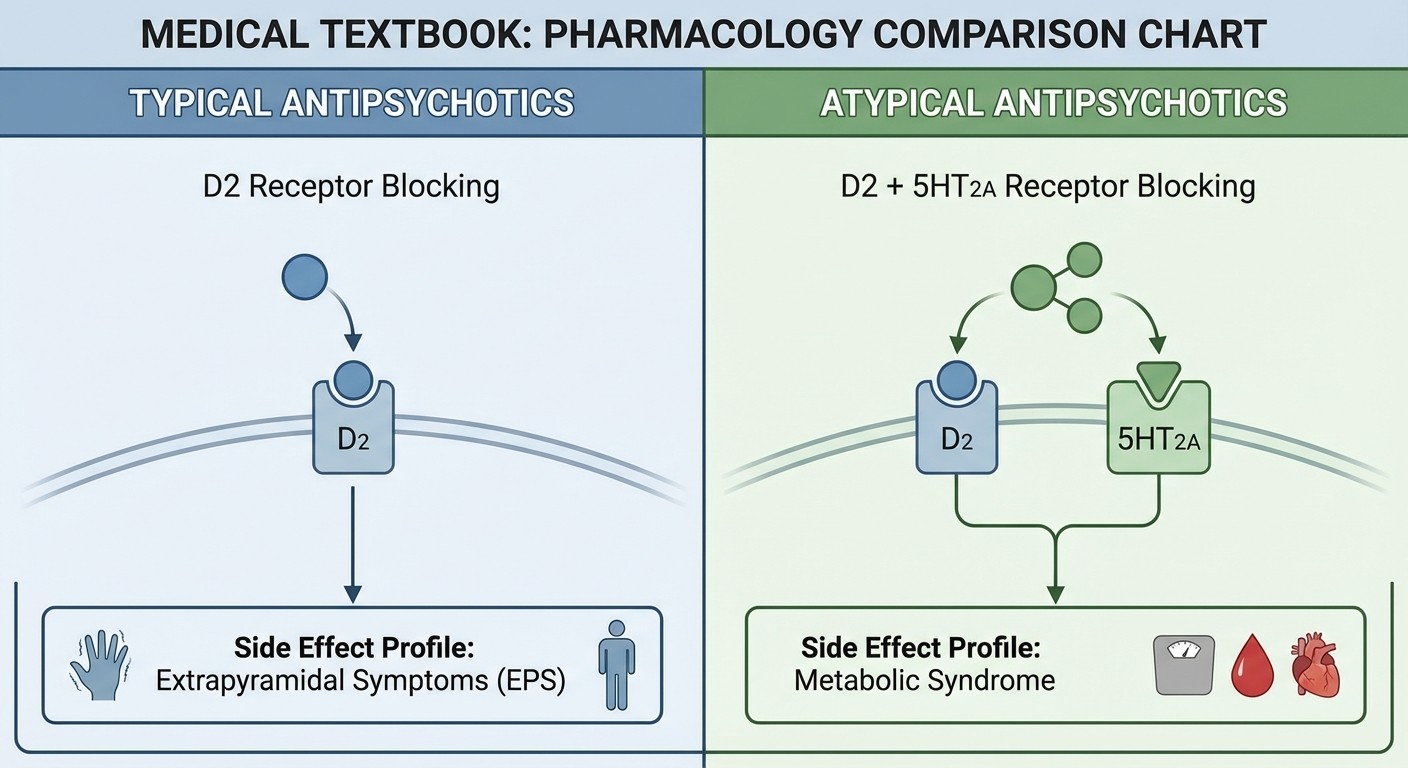
Typical Antipsychotics (First-Generation)
High-Yield Drugs: Haloperidol, Chlorpromazine, Fluphenazine Mechanism: D2 dopamine receptor antagonism (primarily in nigrostriatal and tuberoinfundibular pathways) Mnemonic for extrapyramidal side effects: "PARK the Typical antipsychotics"
Parkinsonism (bradykinesia, rigidity, tremor)
Akathisia (restlessness)
Reactive dystonia (acute muscle spasms)
Kinesia tarda (tardive dyskinesia)
MCQ Pattern: NEET PG consistently tests haloperidol for acute psychotic episodes and its high extrapyramidal side effect profile.
Atypical Antipsychotics (Second-Generation)
High-Yield Drugs: Olanzapine, Risperidone, Quetiapine, Aripiprazole, Clozapine Mechanism: D2 antagonism plus 5-HT2A antagonism, varying receptor profiles Mnemonic for atypical advantages: "Atypical = Anti-EPS, Typical metabolic troubles"
Lower extrapyramidal side effects
Higher metabolic side effects (weight gain, diabetes, dyslipidemia)
Drug-Specific Pearls:
Clozapine: Gold standard for treatment-resistant schizophrenia, requires weekly CBC monitoring for agranulocytosis
Aripiprazole: Partial dopamine agonist, lower metabolic side effects
Quetiapine: Sedating, used off-label for insomnia (controversial)
Study specific mechanisms with our antipsychotics pharmacology lessons and test your knowledge with targeted practice questions.
Antiepileptics: Balancing the Electrical Storm
Sodium Channel Blockers
High-Yield Drugs: Phenytoin, Carbamazepine, Lamotrigine, Valproate Mechanism: Block voltage-gated sodium channels, preventing repetitive neuronal firing Mnemonic for phenytoin side effects: "Phenytoin = Problematic Hair, Problematic Gums"
Hirsutism (excessive hair growth)
Gingival hyperplasia
Also: diplopia, ataxia, nystagmus
Carbamazepine specifics:
First-line for trigeminal neuralgia
Autoinduction of metabolism (dose needs adjustment)
Mnemonic: "Carbamazepine = Car needs Maintenance (autoinduction), Cures facial pain"
Access detailed mechanisms in our CNS antiepileptics lessons and practice with specialized questions.
GABA Enhancers
High-Yield Drugs: Benzodiazepines (Diazepam, Lorazepam), Barbiturates (Phenobarbital), Vigabatin Mechanism: Enhance GABA-mediated inhibition through different pathways Benzodiazepine mnemonic: "Benzo = Better for Status epilepticus"
Lorazepam or diazepam for status epilepticus
Work at GABA-A receptor allosteric site
Side effects: Sedation, tolerance, dependence
Vigabatin pearl: Irreversible GABA transaminase inhibitor, causes retinal toxicity requiring ophthalmologic monitoring.
Calcium Channel Modulators
High-Yield Drugs: Ethosuximide, Gabapentin, Pregabalin Ethosuximide: T-type calcium channel blocker
Specific use: Absence seizures only
Mnemonic: "Etho-SUX-imide = SUcks up absence seizures"
Gabapentin/Pregabalin: Alpha-2-delta subunit blockers
Clinical uses: Neuropathic pain, fibromyalgia, epilepsy
Side effects: Dizziness, somnolence, peripheral edema
Unique Mechanisms
Levetiracetam: SV2A protein modulator
Advantage: Minimal drug interactions
Side effect: Behavioral changes, irritability
Topiramate: Multiple mechanisms (sodium channels, GABA enhancement, glutamate antagonism)
Unique side effects: Kidney stones, weight loss, acute angle-closure glaucoma
Mnemonic: "Topiramate = Top causes Stones, Slim patients, Sudden blindness"
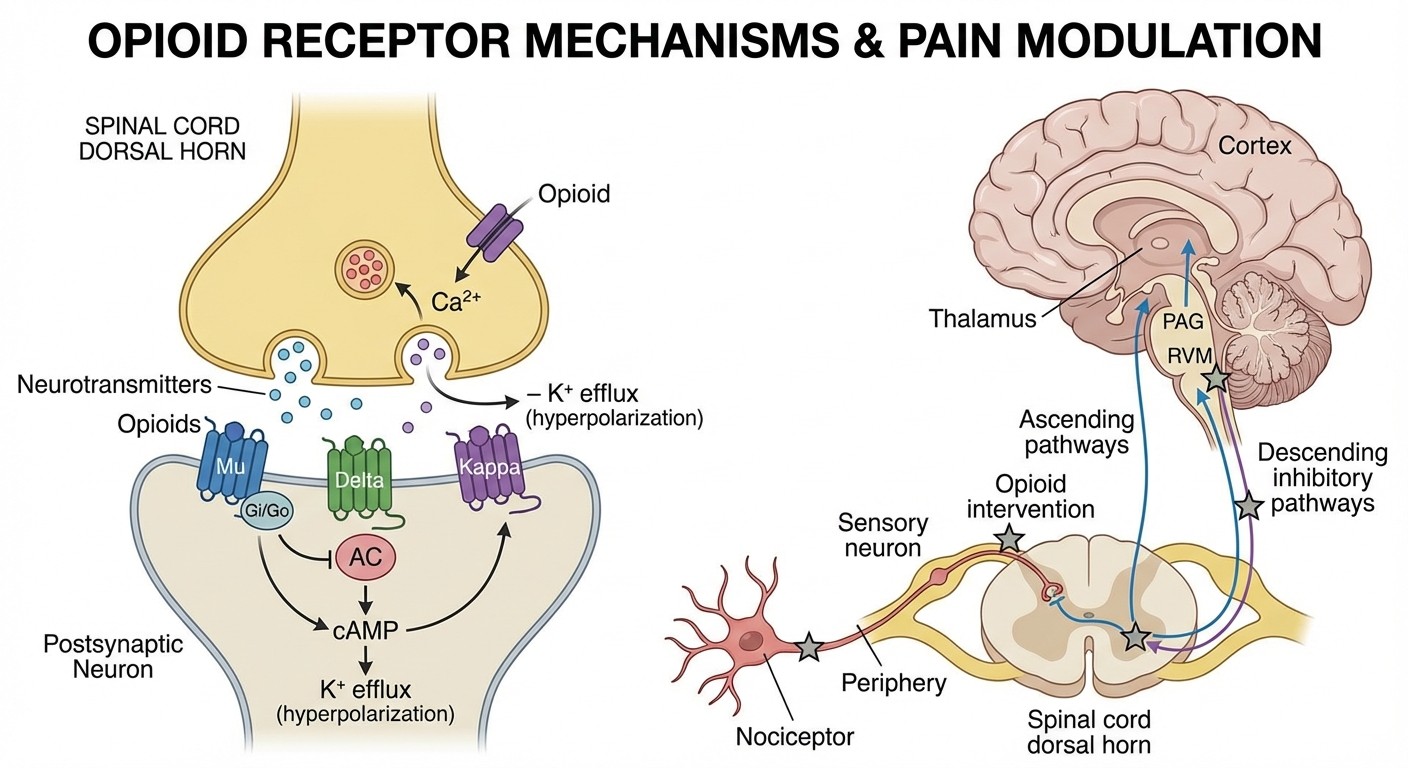
Opioids: The Pain Pathway Players
Opioid Receptor Types
Mechanism overview: Opioids work through mu (μ), delta (δ), and kappa (κ) receptors, all G-protein coupled receptors causing inhibition. Mnemonic for receptor functions: "MuDy Kappa"
Mu (μ): Morphine-like effects (analgesia, euphoria, respiratory depression)
Delta (δ): Depression of respiration, analgesia
Kappa (κ): Ketamine-like dissociation, less euphoria
Strong Opioids
Morphine: Prototype mu-opioid agonist
Active metabolite: Morphine-6-glucuronide (more potent than morphine)
Contraindications: Renal failure (accumulation of metabolites)
Fentanyl: 100x more potent than morphine
Advantage: No histamine release, better for cardiac patients
Route: Transdermal patches for chronic pain
Methadone: Long half-life (15-60 hours)
Clinical use: Opioid addiction maintenance therapy
MCQ trap: Also blocks NMDA receptors
Master opioid pharmacology with our comprehensive opioid analgesics lessons and test your understanding with practice MCQs.
Weak Opioids
Codeine: Prodrug converted to morphine by CYP2D6
Clinical pearl: 10% of population lacks CYP2D6 (poor metabolizers) - codeine ineffective
Use: Mild-moderate pain, cough suppression
Tramadol: Weak mu-opioid agonist + SNRI properties
Advantage: Lower addiction potential
Contraindication: Seizure disorders
Opioid Antagonists
Naloxone: Short-acting mu-opioid antagonist
Use: Opioid overdose reversal
Duration: 30-90 minutes (shorter than most opioids - may need repeat doses)
Naltrexone: Long-acting antagonist
Use: Opioid and alcohol dependence
Mnemonic: "NalTREXone = TREatment for addiction"
High-Yield MCQ Patterns and Mnemonics
Cross-Drug Class Mnemonics
Drug-induced movement disorders: "HALT for movement"
Haloperidol causes parkinsonism
Amiodarone causes tremor
Lithium causes tremor
Tetracycline causes pseudotumor cerebri
Seizure-inducing drugs: "CITB causes seizures"
Clozapine
Isoniazid
Tramadol
Bupropion
Need more memory techniques? Our Synapses feature creates personalized mnemonics for any pharmacology topic, helping you remember complex drug interactions and mechanisms.
NEET PG Favorites
Most tested drug interactions: 1. Phenytoin + Warfarin: Phenytoin induces warfarin metabolism 2. MAOIs + SSRIs: Serotonin syndrome risk 3. Lithium + ACE inhibitors: Lithium toxicity Most tested side effect questions: 1. Clozapine: Agranulocytosis 2. Phenytoin: Gingival hyperplasia 3. Haloperidol: Tardive dyskinesia
Clinical Correlations Table
Drug Class | First-Line Indication | Major Toxicity | Monitoring Required |
|---|---|---|---|
SSRIs | Major depression | Serotonin syndrome | None routine |
Haloperidol | Acute psychosis | Extrapyramidal symptoms | None routine |
Phenytoin | Focal seizures | Gingival hyperplasia | Serum levels |
Morphine | Severe pain | Respiratory depression | Respiratory rate |
Clozapine | Treatment-resistant schizophrenia | Agranulocytosis | Weekly CBC |
For personalized study plans covering all these mechanisms, try Rezzy AI, which adapts to your knowledge gaps in CNS pharmacology and creates custom practice sessions.
Quick Reference: Drug Elimination
Zero-order kinetics (capacity-limited):
Phenytoin at high doses
Ethanol
Salicylates at high doses
First-order kinetics (most drugs):
Half-life determines dosing frequency
5 half-lives for steady state
Mnemonic: "PES drugs have Zero-order elimination at high doses"
Frequently Asked Questions
Which antidepressant is safest in pregnancy?
Sertraline is considered first-line in pregnancy. Paroxetine is contraindicated due to cardiac defects risk. For comprehensive reproductive pharmacology, check our pharmacology flashcards.
What's the difference between tardive dyskinesia and acute dystonia?
Acute dystonia occurs within hours-days of starting antipsychotics (reversible with anticholinergics). Tardive dyskinesia develops after months-years (often irreversible). Remember: "Acute is Early and Easily treated, Tardive is Terrible and permanent."
Which antiepileptic is best for pregnancy?
Lamotrigine has the best safety profile in pregnancy. Valproate has the highest teratogenic risk. Folate supplementation is crucial with all antiepileptics.
How do you reverse opioid overdose?
Naloxone 0.4-2mg IV/IM, may need to repeat due to shorter half-life than most opioids. Duration of action is 30-90 minutes. Always monitor for re-narcotization.
Which psychiatric drug requires blood monitoring?
Clozapine requires weekly CBC for the first 6 months due to agranulocytosis risk (1-2%). Lithium requires serum levels and renal function monitoring.
What's the mechanism of serotonin syndrome?
Excess serotonergic activity causing the triad: altered mental status, neuromuscular hyperactivity (clonus, hyperreflexia), and autonomic instability (hyperthermia, tachycardia). Most commonly occurs with SSRI + MAOI combinations.
Prepare smarter with Oncourse AI — adaptive MCQs, spaced repetition, and AI explanations built for NEET PG. Download free on Android and iOS.