Anatomy
2 questionsThe patient is presenting with pain around the base of the thumb. Which tendons are likely involved?
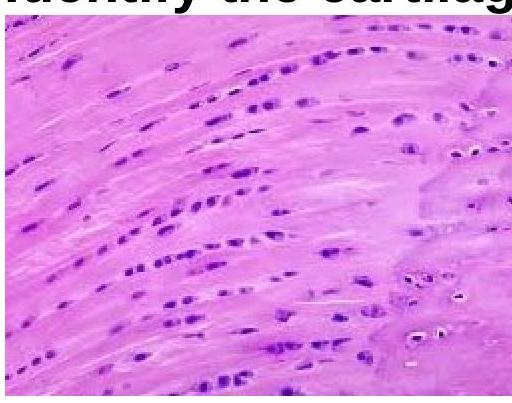
Identify the type of cartilage shown in the image.
Community Medicine
2 questionsWhich of the following diseases is primarily water-related?
As per the Sustainable Development Goals, what is the target for Maternal Mortality Ratio (MMR)?
Internal Medicine
1 questionsEsophageal manometry was performed - it revealed panesophageal pressurization with distal contractile integrity as >450mm Hg pressure in the body. What will be the diagnosis?
Microbiology
1 questionsWhich antibody is not transmitted from mother to baby?
Physiology
2 questionsA 35-year-old female experiences a tingling sensation in her arm after watching TV for long hours with her hands under her head. Which type of nerve fibers is most likely to be affected due to this position?
Which of the following is referred to as the "Window of the limbic system"?
Surgery
2 questionsIn a patient with parathyroid adenoma, how do we confirm the removal of the correct gland after surgery?
A pregnant female had meconium-stained liquor and underwent emergency LSCS. A few days later, her condition deteriorated, and an ultrasound showed edematous bowels. What is the most likely cause of her condition?