Anatomy
1 questionsTumour of the uncinate process of the pancreas will compress which artery
Anesthesiology
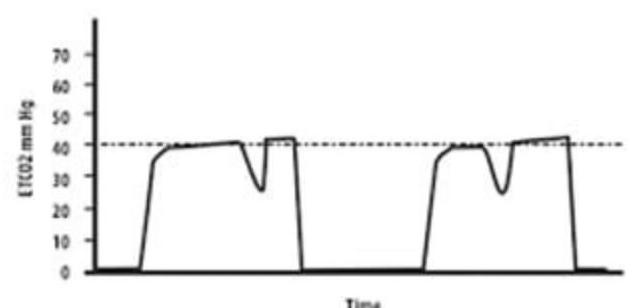
1 questionsWhat does the image of the Capnograph depict?
Internal Medicine
1 questionsWhat is the cause of loss of pain and temperature sensation on the ipsilateral face and contralateral body due to thrombosis?
Microbiology
1 questionsHBsAg is based on which principle
Obstetrics and Gynecology
1 questionsA sexually active female presenting with profuse frothy foul-smelling discharge with intense itching. Strawberry cervix revealed on examination. What will be the diagnosis?
Ophthalmology
1 questionsA 65-year-old male with a history of hypertension and diabetes presents to the OPD with complaints of diplopia and squint. On examination, the secondary deviation is more than the primary deviation. Which of the following is the most likely diagnosis?
Pharmacology
2 questionsWhich of the following drugs can be given in patients of primary pulmonary hypertension?
A patient diagnosed with Rheumatoid arthritis was on medications. After 2 years, he developed a blurring vision and was found to have corneal opacity. Which drug is most likely to cause this?
Physiology
1 questionsWhat is the reflex in which there is inhibition of gastric emptying when there is acid and hypertonic solution in the duodenum?
Surgery
1 questionsA middle-aged man presents with a swelling in the neck that has been present since childhood. The swelling has a bag or worm-like appearance and features a central black spot. Based on this description, what is the most likely diagnosis?