Anatomy
1 questionsTesticular artery is a branch of -
Community Medicine
1 questionsWHO global target for prevention and control of non communicable diseases by 2025 is to decrease the prevalence of raised blood pressure (hypertension) by
Internal Medicine
2 questionsWhich of the following conditions is most commonly associated with cryoglobulinemia?
Which of the following is seen in Rheumatoid Arthritis?
Microbiology
1 questionsMost common catheter-related bloodstream infection is due to:
Obstetrics and Gynecology
1 questionsIn uterine prolapse, how do you assess if a pessary ring is properly in place?
Pathology
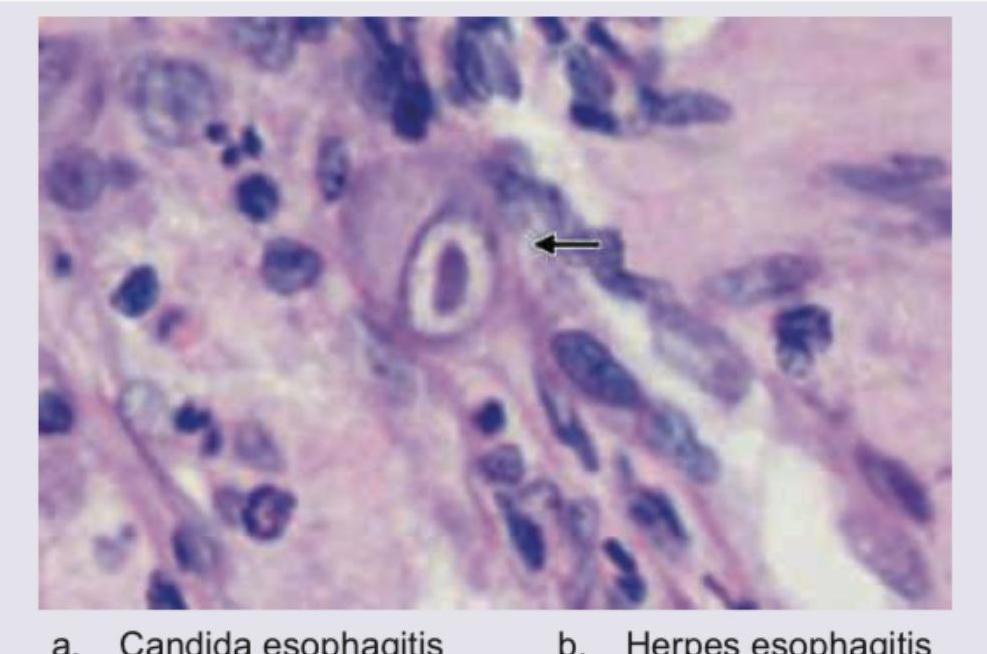
2 questionsA 40-year-old immunocompromised patient presents with complaints of dysphagia. UGI endoscopy shows multiple ulcers in distal esophagus. Biopsy was performed and histopathology is shown below. Diagnosis is:
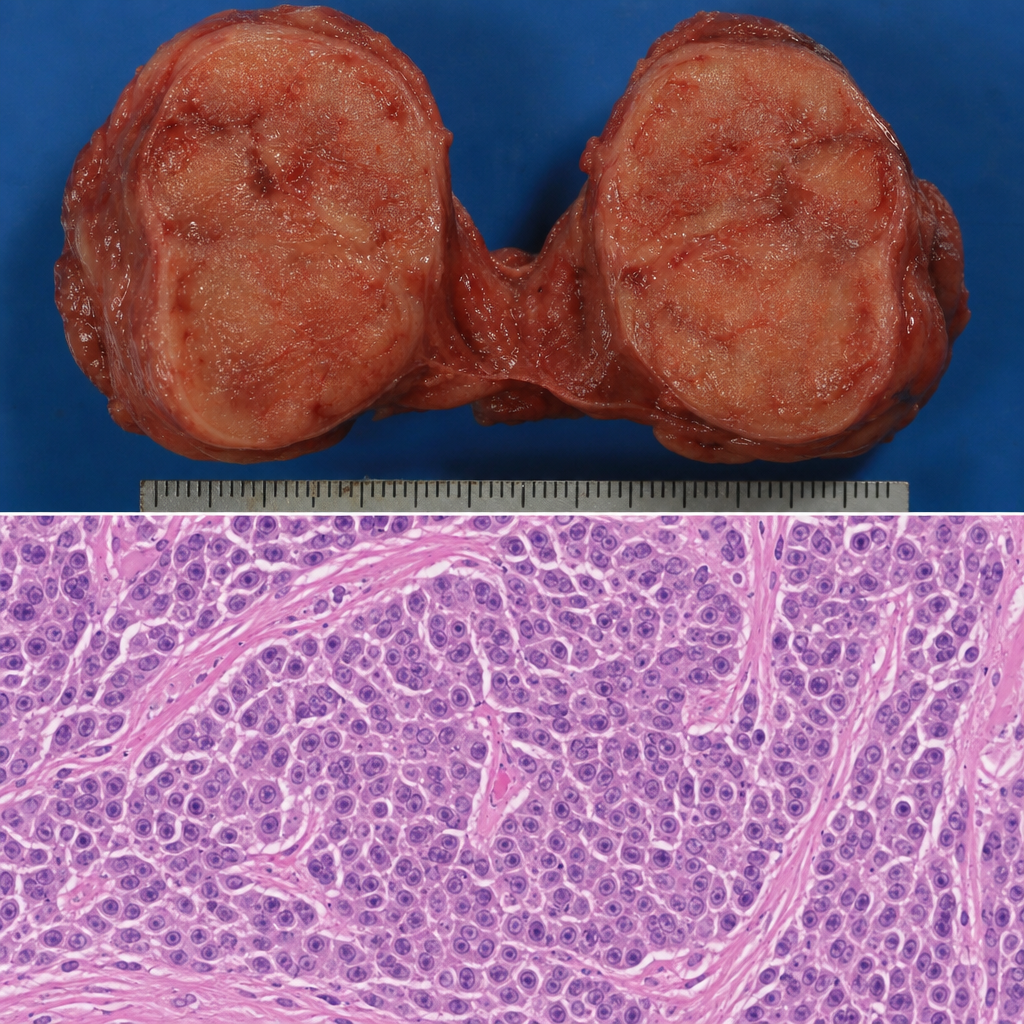
A 50-year-old lady with thyroid swelling underwent total thyroidectomy. The gross specimen and histopathological slide is shown below. Diagnosis is:
Pharmacology
1 questionsWhat is the mechanism of action of colchicine in acute gout?
Psychiatry
1 questionsWhich of the following feature differentiates delirium from dementia?