In a patient with high clinical suspicion of pulmonary thromboembolism, best investigation would be?
Air bronchogram on chest X-ray denotes -
Which of the following is NOT a typical differential diagnosis for a solitary pulmonary nodule?
What is the most common feature of sarcoidosis on chest X-ray?
Investigation with least radiation dose in the diagnosis of Meckel's diverticulum is -
What condition is indicated by the double bubble sign on an abdominal X-ray?
What is an X-ray artifact?
Which of the following conditions is the MOST COMMON cause of rib notching?
For pericardial calcifications, which is the best investigation?
Barium swallow is used for -
NEET-PG 2013 - Radiology NEET-PG Practice Questions and MCQs
Question 31: In a patient with high clinical suspicion of pulmonary thromboembolism, best investigation would be?
- A. D-dimer
- B. CT angiography (Correct Answer)
- C. Catheter angiography
- D. Color Doppler
Explanation: ***CT angiography*** - In a patient with **high clinical suspicion** of pulmonary embolism (PE), CT angiography of the pulmonary arteries is the preferred and often definitive diagnostic test. - It allows for direct visualization of thrombi within the pulmonary arterial tree with high sensitivity and specificity. *D-dimer* - While useful for **ruling out PE** in patients with low or intermediate pre-test probability, a positive D-dimer is non-specific and requires further investigation in high-suspicion cases. - It has a high **negative predictive value** but a low positive predictive value, meaning a normal D-dimer makes PE unlikely, but an elevated one does not confirm it. *Catheter angiography* - This is an **invasive procedure** that is typically reserved for cases where CT angiography is inconclusive or contraindicated, or when interventional treatment is contemplated. - It carries risks such as **bleeding** and **contrast-induced nephropathy**, making it less appropriate as a first-line diagnostic in most situations. *Color Doppler* - Color Doppler ultrasound is primarily used to diagnose **deep vein thrombosis (DVT)** in the lower extremities, which is a common source of PE. - It is **not used to directly diagnose PE** in the pulmonary arteries; however, finding a DVT can support the diagnosis of PE indirectly.
Question 32: Air bronchogram on chest X-ray denotes -
- A. Intrapulmonary lesion (Correct Answer)
- B. Extrapulmonary lesion
- C. Intrathoracic lesion
- D. Extrathoracic lesion
Explanation: ***Intrapulmonary lesion*** - An **air bronchogram** indicates that the air-filled bronchi are surrounded by consolidated or fluid-filled alveoli, making the bronchi visible against the opacified lung parenchyma. - This pattern is a strong sign of a process **within the lung tissue itself**, such as pneumonia, pulmonary edema, or malignancy. *Extrapulmonary lesion* - **Extrapulmonary lesions**, such as pleural effusions or masses originating from the chest wall, typically displace or compress the lung and bronchi, rather than filling the alveoli around them. - They usually do **not produce an air bronchogram** because the air in the bronchi is not juxtaposed against diseased lung parenchyma. *Intrathoracic lesion* - This is a broad term that includes all lesions within the thoracic cavity, both intrapulmonary and extrapulmonary. - While an air bronchogram is an intrathoracic finding, it specifically points to an **intrapulmonary process**, not just any intrathoracic lesion. *Extrathoracic lesion* - **Extrathoracic lesions** are located outside the chest cavity and would not manifest as an air bronchogram on a chest X-ray. - This option is **completely unrelated** to the interpretation of an air bronchogram.
Question 33: Which of the following is NOT a typical differential diagnosis for a solitary pulmonary nodule?
- A. Tuberculoma
- B. Hamartoma
- C. Mycetoma (Correct Answer)
- D. Bronchogenic carcinoma
Explanation: ***Mycetoma*** - A mycetoma is a **fungal infection** that typically affects subcutaneous tissues, skin, and bone, forming granulomas and sinuses. It is not typically seen as a solitary pulmonary nodule. - While pulmonary fungal infections can occur, a mycetoma in the lung typically presents as a **fungus ball (aspergilloma)** within a pre-existing cavity, rather than a solitary, solid nodule. *Tuberculoma* - A tuberculoma is a **granuloma** caused by Mycobacterium tuberculosis, which can present as a well-defined, solitary pulmonary nodule or mass on imaging. - It represents a contained form of tuberculosis and is a common differential for a solitary pulmonary nodule, especially in endemic areas. *Hamartoma* - A hamartoma is a **benign tumor-like malformation** composed of normal tissues (like cartilage, fat, and muscle) that are disorganized. - It is one of the most common benign causes of a solitary pulmonary nodule. *Bronchogenic carcinoma* - Bronchogenic carcinoma, including adenocarcinoma, squamous cell carcinoma, and large cell carcinoma, is the most significant concern when evaluating a solitary pulmonary nodule. - It is a primary **malignant lung tumor** and represents a crucial differential diagnosis due to its poor prognosis if not detected and treated early.
Question 34: What is the most common feature of sarcoidosis on chest X-ray?
- A. Bilateral hilar lymphadenopathy (Correct Answer)
- B. Cavitation
- C. Pleural effusion
- D. Reticular opacities
Explanation: ***Bilateral hilar lymphadenopathy*** - **Bilateral hilar lymphadenopathy** is the hallmark radiological feature of sarcoidosis, seen in over 75% of cases. - This finding, often symmetrical, represents the accumulation of **non-caseating granulomas** in the lymph nodes. - Classic presentation in **Stage I and Stage II** sarcoidosis. *Pleural effusion* - **Pleural effusions** are uncommon in sarcoidosis, occurring in less than 5% of cases. - When present, they are usually small and unilateral, and their presence should prompt consideration of alternative diagnoses. *Cavitation* - **Cavitation** is a rare manifestation of sarcoidosis and is more characteristic of infectious processes like **tuberculosis** or certain fungal infections. - If seen, it usually suggests severe parenchymal involvement or superimposed infection. *Reticular opacities* - While **reticular opacities** (interstitial changes) can be seen in later stages of sarcoidosis, representing **pulmonary fibrosis**, they are not the *most common* initial finding. - These opacities indicate chronic disease progression (Stage III/IV) rather than the initial presentation.
Question 35: Investigation with least radiation dose in the diagnosis of Meckel's diverticulum is -
- A. MRI
- B. CT
- C. Contrast radiography
- D. Technetium -99m scanning (Correct Answer)
Explanation: ***Technetium-99m scanning*** - **Technetium-99m pertechnetate scan** (Meckel's scan) is the **gold standard investigation** for diagnosing Meckel's diverticulum with ectopic gastric mucosa - Among the investigations that can actually **diagnose Meckel's diverticulum**, it has the **lowest radiation dose** (approximately 1-2 mSv) - The radioisotope is specifically taken up by ectopic gastric mucosa, providing both diagnostic utility and relatively low radiation exposure - **Sensitivity: 85-95%** for detecting ectopic gastric mucosa in Meckel's diverticulum - The radiation dose is comparable to a few months of natural background radiation and significantly lower than CT or contrast studies *MRI* - While **MRI uses no ionizing radiation**, it is **not a standard or practical investigation** for diagnosing Meckel's diverticulum - MRI cannot identify ectopic gastric mucosa specifically - It is rarely used in clinical practice for this indication - The question asks about investigation "in the diagnosis" of Meckel's diverticulum, implying a test that is actually used diagnostically *CT* - **Computed Tomography (CT)** delivers a **high radiation dose** (typically 5-10 mSv or more) - While it can identify structural abnormalities, it is not specific for Meckel's diverticulum - Not the first-line investigation for this condition *Contrast radiography* - **Contrast studies** (barium studies) use **moderate ionizing radiation** (3-5 mSv) - Limited utility in diagnosing Meckel's diverticulum as it primarily assesses luminal patency - Cannot identify ectopic gastric mucosa - Lower sensitivity compared to Tc-99m scanning
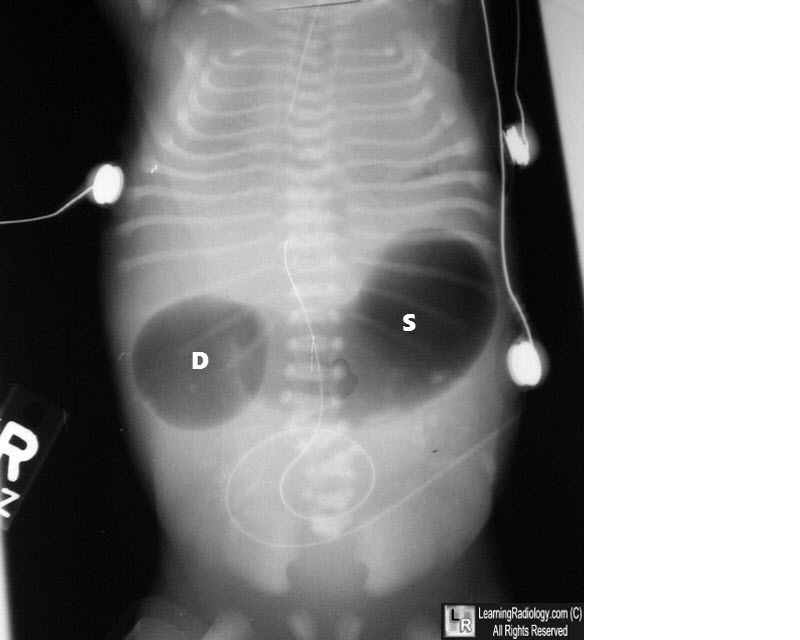
Question 36: What condition is indicated by the double bubble sign on an abdominal X-ray?
- A. Duodenal stenosis
- B. Volvulus
- C. All of the options
- D. Duodenal atresia (Correct Answer)
Explanation: ***Duodenal atresia*** - The **double bubble sign** on an abdominal X-ray is pathognomonic for **duodenal atresia**, characterized by two air-filled bubbles: one in the stomach and one in the proximal duodenum, separated by the pylorus. - This congenital anomaly results from a complete obstruction of the duodenum, preventing the passage of air and fluid past this point. *Duodenal stenosis* - While also an obstruction of the duodenum, **duodenal stenosis** is an incomplete obstruction, meaning some gas will pass beyond the duodenum. - This would result in gas being present in the distal bowel, which is not seen with a classic "double bubble" where the bowel distal to the duodenum is gasless. *Volvulus* - **Volvulus** involves the twisting of a loop of intestine, leading to obstruction and potentially ischemia. - While it can cause obstruction, it typically presents with a "corkscrew" appearance on an upper GI series or signs of diffuse bowel distension, not the isolated double bubble. *All of the options* - The double bubble sign is highly specific to **duodenal atresia** due to the complete obstruction it signifies. - Other conditions like duodenal stenosis and volvulus cause different radiological patterns, making this option incorrect.
Question 37: What is an X-ray artifact?
- A. A radiographic finding that indicates disease pathology
- B. A normal anatomical structure visible on X-ray
- C. An image distortion produced when the patient moves during the X-ray procedure
- D. An unwanted image distortion that doesn't represent actual anatomy (Correct Answer)
Explanation: ***An unwanted image distortion that doesn't represent actual anatomy*** - An **X-ray artifact** is any feature or distortion on a radiographic image that is not present in the actual object being imaged. - These can arise from various sources such as patient movement, equipment malfunction, or improper technique, leading to **misinterpretation** of the image. - Artifacts are unwanted findings that can obscure true pathology or mimic disease. *A normal anatomical structure visible on X-ray* - This describes a **true anatomical finding**, which is the intended purpose of an X-ray. - Normal anatomical structures are expected and assist in diagnosis, unlike artifacts which obscure or mimic pathology. *An image distortion produced when the patient moves during the X-ray procedure* - While **patient motion** is a common cause of X-ray artifacts, this describes just one specific type (motion artifact), not a comprehensive definition of what an artifact is. - Other sources like metallic objects, scatter radiation, or detector issues can also cause artifacts. *A radiographic finding that indicates disease pathology* - This describes **true pathology** or disease findings, which is what radiologists aim to identify. - Artifacts are the opposite - they are false findings that do not represent actual anatomy or pathology.
Question 38: Which of the following conditions is the MOST COMMON cause of rib notching?
- A. Coarctation of aorta (Correct Answer)
- B. Atrial septal defect
- C. Chronic superior venacava obstruction
- D. Congenital interruption of aorta
Explanation: ***Coarctation of aorta*** - **Coarctation of the aorta** is the classic and **most common cause** of rib notching. - The notching is caused by the enlargement and tortuosity of the **intercostal arteries** as they provide collateral circulation to bypass the narrowed aorta. *Chronic superior venacava obstruction* - Chronic superior vena cava (SVC) obstruction may lead to the development of collateral circulation through the azygos and hemiazygos veins, but it does **not typically cause rib notching**. - Rib notching is specifically related to collateral flow bypassing an aortic obstruction, not a venous obstruction. *Atrial septal defect* - An **atrial septal defect (ASD)** is a communication between the atria that can lead to right heart volume overload and pulmonary hypertension. - While it's a congenital heart defect, an ASD does **not cause rib notching** as it does not involve an obstruction of systemic arterial flow requiring collateral circulation via the intercostal arteries. *Congenital interruption of aorta* - While **congenital interruption of the aorta** also involves an aortic obstruction, it is a **much rarer condition** than coarctation of the aorta. - Due to its rarity, it is not considered the most common cause of rib notching, even though it would theoretically lead to similar collateral vessel formation.
Question 39: For pericardial calcifications, which is the best investigation?
- A. Ultrasound
- B. CT scan (Correct Answer)
- C. MRI
- D. Transesophageal echocardiography
Explanation: ***Correct: CT scan*** - **CT scans** are highly sensitive and specific for detecting **pericardial calcifications** due to their excellent spatial resolution and ability to measure calcium density (Hounsfield units). - They provide detailed anatomical information about the **pericardium** and can accurately map the extent, location, and thickness of calcified areas. - **CT is the gold standard** for detecting and quantifying pericardial calcification, particularly in constrictive pericarditis. *Incorrect: Ultrasound* - While ultrasound (echocardiography) can visualize the pericardium and may detect calcifications, its ability to definitively identify and characterize **calcifications** is limited compared to CT. - **Acoustic shadowing** from calcifications can obscure underlying structures, making a precise assessment challenging. - Useful for detecting pericardial effusion and thickening, but not optimal for calcification assessment. *Incorrect: MRI* - **MRI excels** in visualizing soft tissues, pericardial inflammation, and fluid collections, but it is **poor at detecting calcium**. - Calcifications typically appear as signal voids (black) on MRI, making it difficult to differentiate them from other structures, air, or motion artifacts. - MRI is valuable for assessing pericardial inflammation and constriction but not the preferred method for calcification. *Incorrect: Transesophageal echocardiography* - TEE offers high-resolution images of cardiac structures and is primarily used for assessing valve function, intracardiac masses, endocarditis, and aortic pathology. - Its utility in detecting and characterizing **pericardial calcifications** is limited compared to CT, especially for diffuse or subtle calcifications. - The pericardium is not optimally visualized with TEE compared to transthoracic echocardiography.
Question 40: Barium swallow is used for -
- A. Colon
- B. Esophagus (Correct Answer)
- C. Duodenum
- D. Jejunum
Explanation: ***Esophagus*** - A **barium swallow** specifically visualizes the **esophagus**, pharynx, and sometimes the early stomach. - It's used to identify abnormalities like **dysphagia**, strictures, **achalasia**, or tumors by coating the mucosal lining. *Colon* - The colon is typically examined using a **barium enema**, where barium sulfate is administered rectally. - This procedure is effective for visualizing the large intestine for conditions like **polyps**, diverticula, or inflammatory bowel disease. *Duodenum* - While a barium swallow may transiently show the **duodenum**, its primary target is the esophagus and stomach. - More detailed imaging of the duodenum often requires an **upper GI series (UGI)**, which is a broader study of the upper digestive tract. *Jejunum* - The jejunum is part of the small intestine and is best visualized through a **small bowel follow-through (SBFT)** procedure. - This involves ingesting barium and taking serial X-rays as it progresses through the small bowel, to detect conditions like **Crohn's disease** or obstructions.